Download
1 / 14
160 likes | 274 Views
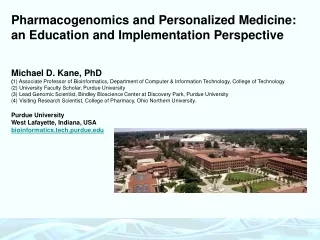
Pharmacogenomics and Personalized Medicine. Michael D. Kane, PhD Associate Professor, University Faculty Scholar, Graduate Education Chair Department of Computer and Information Technology College of Technology & Lead Genomic Scientist, Bindley Bioscience Center at Discovery Park

E N D
Pharmacogenomics and Personalized Medicine Michael D. Kane, PhD Associate Professor, University Faculty Scholar, Graduate Education Chair Department of Computer and Information Technology College of Technology & Lead Genomic Scientist, Bindley Bioscience Center at Discovery Park Purdue University West Lafayette, Indiana 47907 bioinformatics.tech.purdue.edu Current Industry Positions: Co-Founder: Genomic Guidance, LLC (Personalized Medicine, Information Management) Co-Founder: Broadband Antenna Tracking Systems, Inc (Wireless Communications Technology) Former Industry Positions: Co-Founder & President: Nucleico, LLC (Gene Expression Profiling, Microarrays) VP of R&D: Genomic Solutions, Inc (Biotechnology Instrumentation and Software, Microarrays) Senior Scientist: Pfizer Pharmaceuticals (Molecular Technologies Group) Scientific Advisor and Co-Inventor: Sensigen Diagnostics (Clinical HPV Detection)
Bioinformatics & Genomics From Genetics to Data Management Systems… >gi|1924939|emb|X98411.1|HSMYOSIE Homo sapiens partial mRNA for myosin-IF CAGGAGAAGCTGACCAGCCGCAAGATGGACAGCCGCTGGGGCGGGCGCAGCGAGTCCATCAATGTGACCC TCAACGTGGAGCAGGCAGCCTACACCCGTGATGCCCTGGCCAAGGGGCTCTATGCCCGCCTCTTCGACTT CCTCGTGGAGGCCATCAACCGTGCTATGCAGAAACCCCAGGAAGAGTACAGCATCGGTGTGCTGGACATT TACGGCTTCGAGATCTTCCAGAAAAATGGCTTCGAGCAGTTTTGCATCAACTTCGTCAATGAGAAGCTGC AGCAAATCTTTATCGAACTTACCCTGAAGGCCGAGCAGGAGGAGTATGTGCAGGAAGGCATCCGCTGGAC TCCAATCCAGTACTTCAACAACAAGGTCGTCTGTGACCTCATCGAAAACAAGCTGAGCCCCCCAGGCATC ATGAGCGTCTTGGACGACGTGTGCGCCACCATGCACGCCACGGGCGGGGGAGCAGACCAGACACTGCTGC AGAAGCTGCAGGCGGCTGTGGGGACCCACGAGCATTTCAACAGCTGGAGCGCCGGCTTCGTCATCCACCA CTACGCTGGCAAGGTCTCCTACGACGTCAGCGGCTTCTGCGAGAGGAACCGAGACGTTCTCTTCTCCGAC CTCATAGAGCTGATGCAGTCCAGTGACCAGGCCTTCCTCCGGATGCTCTTCCCCGAGAAGCTGGATGGAG ACAAGAAGGGGCGCCCCAGCACCGCCGGCTCCAAGATCAAGAAACAAGCCAACGACCTGGTGGCCACACT GATGAGGTGCACACCCCACTACATCCGCTGCATCAAACCCAACGAGACCAAGCACGCCCGAGACTGGGAG GAGAACAGAGTCCAGCACCAGGTGGAATACCTGGGCCTGAAGGAAAACATCAGGGTGCGCAGAGCCGGCT TCGCCTACCGCCGCCAGTTCGCCAAATTCCTGCAGAGGTATGCCATTCTGACCCCCGAGACGTGGCCGCG GTGGCGTGGGGACGAACGCCAGGGCGTCCAGCACCTGCTTCGGGCGGTCAACATGGAGCCCGACCAGTAC CAGATGGGGAGCACCAAGGTCTTTGTCAAGAACCCAGAGTCGCTTTTCCTCCTGGAGGAGGTGCGAGAGC GAAAGTTCGATGGCTTTGCCCGAACCATCCAGAAGGCCTGGCGGCGCCACGTGGCTGTCCGGAAGTACGA GGAGATGCGGGAGGAAGCTTCCAACATCCTGCTGAACAAGAAGGAGCGGAGGCGCAACAGCATCAATCGG AACTTCGTCGGGGACTACCTGGGGCTGGAGGAGCGGCCCGAGCTGCGTCAGTTCCTGGGCAAGAAGGAGC GGGTGGACTTCGCCGATTCGGTCACCAAGTACGACCGCCGCTTCAAGCCCATCAAGCGGGACTTGATCCT GACGCCCAAGTGTGTGTATGTGATTGGGCGAGAGAAGATGAAGAAGGGACCTGAGAAAGGTCCAGTGTGT GAAATCTTGAAGAAGAAATTGGACATCCAGGCTCTGCGGGGGGTCTCCCTCAGCACGCGACAGGACGACT TCTTCATCCTCCAAGAGGATGCCGCCGACAGCTTCCTGGAGAGCGTCTTCAAGACCGAGTTTGTCAGCCT TCTGTGCAAGCGCTTCGAGGAGGCGACGCGGAGGCCCCTGCCCCTCACCTTCAGCGACACACTACAGTTT CGGGTGAAGAAGGAGGGCTGGGGCGGTGGCGGCACCCGCAGCGTCACCTTCTCCCGCGGCTTCGGCGACT TGGCAGTGCTCAAGGTTGGCGGTCGGACCCTCACGGTCAGCGTGGGCGATGGGCTGCCCAAGAACTCCAA GCCTACCGGAAAGGGATTGGCCAAGGGTAAACCTCGGAGGTCGTCCCAAGCCCCTACCCGGGCGGCCCCT GGCGCCCCCCAAGGCATGGATCGAAATGGGGCCCCCCTCTGCCCACAGGGGG
Bioinformatics & Genomics Biomolecular Trends: Yeast Genome Human Genome Onion Genome Lily Genome 1.2 x 107 BP 3.3 x 109 BP 15 x 109 BP 90 x 109 BP (1/275x Human) (1x) (5x Human) (27x Human)
Introduction to PharmacoGenomics Single Nucleotide Polymorphisms (SNPs) are simple changes (or differences) in the DNA sequence that appear to have little or no impact on human health. They represent 90% of all human genetic variations. Genetically similar to a mutation, but distinct in that a SNP is not causal to a clinical disease or disorder (or at least not yet causally linked, and not really applicable to ages >40 yrs old). Across the human genome we average approximately 1 SNP for every 300 base pairs of DNA (over one million known SNPs that occur at a frequency of 1% or higher in the world population). Important Consideration: Inheritance The appearance of deleterious mutations during evolution tend to NOT be inherited for obvious reasons, at least those that affect growth, reproduction and viability. …and our modern existence is the result of millions of years of tolerated (and occasionally beneficial) changes in our genome, which is most often evident in what we can and cannot eat or consume (think: evolutionary pressure & natural selection) Monomethyl Hydrazine (in “False” Morel Mushrooms) Tylenol: Acetaminophen (Cats?) (many examples of “toxins” in nature, many of them are presumably synthesized to prevent consumption or predation of the host plant or organism) Modern drug discovery & development falls outside the tolerances & toxicity that have resulted from evolution, because most of these compounds have NEVER been seen in nature.
Adverse Drug Reactions More than 770,000 patients die or sustain serious injury every year in the U.S. from Adverse Drug Reactions (ADRs). ADRs are therefore the 4th leading cause of death in the United States and are one of the leading, preventable public health issues today. ADRs cost each hospital approximately $5.6 million per year. In terms of total health care dollars, ADRs cost the U.S. health care system between $1.5 and $5.4 billion per year. SNPs have been purposed to account for 24% of all ADRs.
The Pharmacogenomics of Warfarin When you ingest a drug, the drug is absorbed into the circulatory system and is distributed throughout the body. The drug is then available to carry out its intended ‘mechanism of action’ (MOA). In the case of WARFARIN, it inhibits Vitamin K Epoxide Reductase Complex 1 (VKORC1), and reduces blood clotting. It is the largest selling anticoagulant in the world, and the leading case in support of Personalized Medicine”. Subsequently, the body has the ability to eliminate the drug from the body through “drug metabolism”, which is primarily carried out in the liver. WARFARIN is metabolized primarily by the oxidative liver enzyme CYP2C9, which basically adds an oxygen group to the WARFARIN structure thereby inactivating its MOA and increasing its likelihood of elimination from the body via the kidneys (urine). For this reason, drug tests that utilize urine a sample source often look for the “metabolite” of the drug in the urine, rather than the ingested drug. IMPORTANT: If you are prescribed WARFARIN, you have a condition that generates potentially life-threatening blood clots. If you are dosed with too much WARFARIN you could die from complications due to internal bleeding, yet if you are dosed with too little WARFARIN you may be in danger of serious consequences due to circulating embolism.
Go to www.genescription.com Genescription is a free, online training program in Personalized Medicine for instructors and healthcare professionals. (developed through a grant from Microsoft External Research)
Examples of Clinically-Relevant SNPs From: Kane, et al. Drug Safety Assurance through Clinical Genotyping: Near-Term Considerations for a System-Wide Implementation of Personalized Medicine. Personalized Medicine 5(4): 387-397 (2008)
Evidence suggests that Healthcare will be a primary influence on the US economy for the next 50 years. The “Workforce 2015: Strategy Trumps Shortage” describes how hospitals face the overlapping challenges of attracting and retaining replacements for retiring workers, expanding its workforce to care for an aging population, the greater demand for information technology professionals while coping with significant changes in healthcare delivery. The “Global Healthcare Information Technology (2009 - 2014)” report states that the current healthcare information technologymarket is estimated to be $53.8 billion. Where do YOU see professional, commercial, and entrepreneurial opportunities in this emerging area of healthcare?
Clinical Genotyping Workflow in Healthcare From: Kane, et al. Drug Safety Assurance through Clinical Genotyping: Near-Term Considerations for a System-Wide Implementation of Personalized Medicine. Personalized Medicine 5(4): 387-397 (2008)
Clinical Genotyping Workflow in Healthcare From: Kane, et al. Drug Safety Assurance through Clinical Genotyping: Near-Term Considerations for a System-Wide Implementation of Personalized Medicine. Personalized Medicine 5(4): 387-397 (2008)
Considerations for Clinical Genotyping Data Management and User Interface Design and Content in Healthcare From: Kane, et al. Drug Safety Assurance through Clinical Genotyping: Near-Term Considerations for a System-Wide Implementation of Personalized Medicine. Personalized Medicine 5(4): 387-397 (2008)