Download
1 / 31
340 likes | 370 Views
Gastroparesis. Internal Medicine Noon Conference September 16 th , 2019 Charles McMahon, MD. Gastroparesis. Lecture overview: Definitions Normal gastric function Pathophysiology Epidemiology Signs/Symptoms Testing/Diagnosis Treatment. Gastroparesis Definition.

E N D
Gastroparesis Internal Medicine Noon Conference September 16th, 2019 Charles McMahon, MD
Gastroparesis • Lecture overview: • Definitions • Normal gastric function • Pathophysiology • Epidemiology • Signs/Symptoms • Testing/Diagnosis • Treatment
Gastroparesis Definition Delayed emptying of the stomach in the absence of mechanical outlet obstruction ACG guideline definition – “combination of the symptoms of gastroparesis, absence of gastric outlet obstruction or ulceration, and delay in gastric emptying.”
Normal Stomach Mechanical Physiology Stomach is very small when relaxed and empty and increases 10x w/ intake Liquids empty from the stomach first, followed by solids, which are initially stored in the fundus (fundic accommodation – lag phase) Food is then moved from the fundus to the antrum and ground into chyme
Normal Stomach Electrical Physiology • Mediated by the myenteric plexus • Myenteric plexus is regulated via vagal efferents from the dorsal motor vagal complex in the brainstem • Myenteric plexus motor neurons: • Excitatory: Acetylcholine • Inhibitory: NO • Gastric pacemaker – Interstitial Cells of Cajal (ICC), contractile rhythm 3cpm
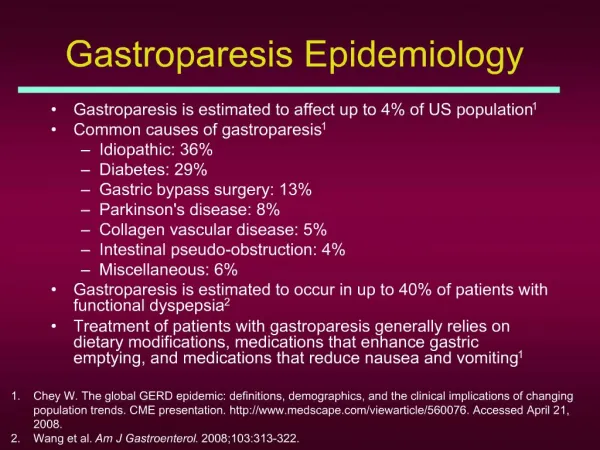
Gastroparesis Epidemiology • Often undiagnosed, true prevalence may be >1.5% • More common in women (approx 4:1 prevalence) • More common in diabetes (30x Type 1, 8x Type II) • Population based studies • 5.2%, 1%, and 0.2% of I, II, and nondiabetics develop gastroparesis
Gastroparesis Epidemiology • Mean onset age 33 • Impacts QOL, costs, and associated with M&M
GastroparesisPathophysiology • Unknown to a significant degree • Full thickness gastric biopsies have shown multiple abnormalities: • ICC dropout (seems to correlate best with delays in gastric emptying) • Decreased density of nerve fibers • Smooth muscle fibrosis • Changes in neurotransmitters • Myenteric immune infiltrate in the muscle layer
GastroparesisPathophysiology • DM – abnormalities on multiple levels – motor dysfunction, intrinsic nervous system damage • Postsurgical • Medication induced (anticholinergic, opiate, GLP-1 analogs) • Postviral Gastroparesis - viral prodrome
Gastroparesis Signs/Symptoms • Clinical suspicion: • Nausea • Vomiting • Bloating • Early satiety/post-prandial fullness • Abdominal pain • Difficult to control/refractory GERD • H/o diabetes, recent viral illness, recent negative EGD and/or upper GI imaging
Gastroparesis Signs/Symptoms • Gastroparesis Cardinal Symptom Index (GCSI)
Gastroparesis Testing/Diagnosis • Concern for gastroparesis: • EGD (r/o ulcer, stricture, other cause of narrowing, H. Pylori, malignancy) • Medication review • Imaging • Pill testing, via pH or direct visualization/Breath testing – not validated currently • Gastric Scintigraphy, Gastric Emptying Study, GES
Gastroparesis Testing/Diagnosis • Gastric Emptying Study: • Nuclear Medicine Test • Scintigraphy at 0, 1, 2, 4 hours w/ radiolabeled food (eggs, generally) • Shorter tests/liquid tests less sensitive • Need to be off meds that accelerate or delay gastric emptying for 48-72h prior to testing and have euglycemia • Positive - >60% label remaining at 2 hours and > 10% at 4 hours
Gastroparesis Testing/Diagnosis • Other, less often used/still somewhat experimental tests: • Wireless capsule motility testing • 13C breath testing
Gastroparesis Testing/Diagnosis • Seems to be poor correlation between symptoms and degree of emptying seen on GES • Screen patients with gastroparesis for DM, thyroid disease – if unknown. Consider autoimmune/neurologic screening
Gastroparesis Testing/Diagnosis • Accelerated/rapid gastric emptying and functional dyspepsia can present with symptoms similar to gastroparesis, so GES is recommended prior to initiating medical or surgical therapies • Differential diagnosis of symptoms can also include rumination syndrome, cyclic vomiting syndrome, and cannabinoid hyperemesis syndrome
Gastroparesis Treatment • Resuscitation/near and long term plan for nutritional support (other enteral feeding options and/or TPN) • Enteral (and postpyloric) feeding preferred • Consultation w/ a dietician • Frequent small volume/fiber/fat meals • Liquids only, if all that is tolerated • Jejunal feeding may be indicated if repeated hospitalizations or 10% BW loss in 3-6 months
Gastroparesis Treatment • Medical: • Prokinetics: Metoclopramide (D2 antagonist) • Try as low dose, short course as possible and document discussion of risks/benefits (TD <1%) • Domperidone (D2 antagonist, not in U.S. w/o investigatory drug form) • Need monitoring of baseline and repeat ECGs • Withhold if QTc >470ms in males and >450ms in females
Gastroparesis Treatment • Medical: • Erythromycin: Macrolide antibiotic (mimics motilin) • Good for acute/hospital treatment • Tachyphylaxis (2 weeks) • Can also prolong QT and interfere w/ drug metabolism • Symptom control w/ Ondansetron (5-HT3 antagonists), Prochlorperazine, Promethazine, Diphenhydramine, Benzos, Tricyclics (more for visceral hypersensitivity) to act on different serotonin, histamine, dopamine, muscarinic, GABA receptors
Gastroparesis Treatment • Avoid/minimize opioids, motility slowing medications • Avoid alcohol, tobacco • Glycemic control (BG <200) • Diet: low fiber/fat/red meat, small and frequent meals • Postviralgastroparesis may improve with time (can be > 1 year)
Gastroparesis Treatment • Non-Medical: • ? Botox injection into pyloric area? • Conflicting study data, not currently recommended • G-POEM • Self Expanding Metal Pyloric Stents • Unclear long term risks and significant complication risk as well as lack of data
Gastroparesis Treatment • Non-Medical: • Gastric Electric Stimulators “gastric pacemakers” (surgical implant, GES) • Compassionate use • Equivocal results – mostly surgical studies • Costs/risks of surgery • Need for careful patient selection (better in DM?) • Sometimes other surgeries – venting gastrostomy, gasctrectomy, pyloroplasty, gastrojejunostomy • Acupuncture
References • Dhalla S, Pasricha, J. Gastroparesis. In: Rao SSC, Parkman HP, McCallum RW. Handbook of gastrointestinal motility and functional disorders. Thorofare, NJ: SLACK Incorporated; 2015 107-114). • Camilleri M, et al. ACG Guidelines. Management of gastroparesis. Am J Gastroenterol 2013; 108:18–37; doi: 10.1038/ajg.2012.373; published online 13 November 2012. Accessed March 18, 2017. • Koch, K. (2015). Gastric Neuromuscular Function and Neuromuscular Disorders (9th ed., pp. 811-838). Philadelphia, Pennsylvania: Elsevier Saunders. • Camilleri M. Treatment of gastroparesis. In: UpToDate, Grover S (Ed), UpToDate, Waltham, MA. (Accessed on March 20, 2017.)