Download
1 / 19
190 likes | 194 Views
This presentation highlights the HIV epidemic in South Sudan, including key populations, vulnerable groups, risk factors, and the response plan.

E N D
HIV in Education in Emergency Presentation to Education Cluster20 October 2014
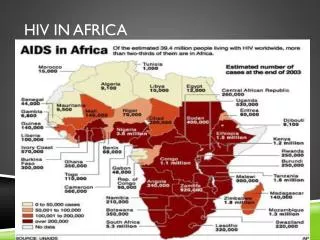
National prevalence: 2.6%
The HIV Epidemic in South Sudan • Mixed epidemic – general population but also: • Akobo, Leer, KajoKejiandMaridihave recorded steady increase in new infections since 2007 Geographic hotspots Ezo = 14% Yambio = 8.4% Tambura = 6.5% Juba = 4.7% Nimule = 4.4% Maridi = 4.1% Key populations Clients of sex workers Uniformed services Casual sex partners Female sex workers Polygamous partners Men who have sex with men
Proportion of new infections by risk group Ref: Modes of Transmission Analysis, 2013
Other vulnerable groups • Prevalence and incidence among women and girls is twice that of men and boys: • Gender inequalities – low status of women and girls, no decision making power, economic inequality • Early sex debut – <15 years: 11% national; 20% in WE; 18% in WBG; 14% in Unity & CE; 11% in EE; 10% in Warrap; 6% in Warrap & NBG; 3% Lakes & UN • Gender based violence – sexual violence, intimate partner violence • Harmful traditional practices – widow inheritance, polygamy (risk of infection is 6 times higher for partners in polygamous relationship) • Male attitudes and behaviours – casual sex/sex workers/multiple partners, low condom use, low male circumcision etc • Risk of mother to child transmission still stands at 29%; 2,400+ new infections in 2013 = 16% of all new infections
Young People • South Sudan is a young population: 72% under 30 years, 51% under 18 years • 20,000 young people <15 years living with HIV • Most young people do not have access to sexual and reproductive health information and services • Risk factors include early sex, inter-generational sex, gender based violence, no access to condoms etc • 2010 KAP study in Greater Equatoria: • 21% early sex debut, mean age of 10.75 • Very low comprehensive knowledge of HIV (11.3%) • Low knowledge of correct condom use (31%)
Risk and Vulnerability Factors Risk Factors • Early sex debut • Low condom use • Low male circumcision • Sex work in urban settings • Multiple sexual partners • Low Knowledge of HIV and HIV prevention methods • GBV including sexual violence • Stigma, denial & discrimination Vulnerability Factors Gender Factors: • Low status of women • Harmful traditional practices • Gender inequalities Humanitarian Factors: • Broken social structures / family • Negative coping mechanisms • Sex work/transactional sex • GBV including sexual violence • Low access to HIV services
Getting to Zero • 10 HLM 2011 Declaration and Targets towards 2015: • Reduce new HIV infections and AIDS-related deaths by 50% • Retargeting towards 2020 - post 2015 towards 2030; focus on treatment as prevention plus prevention targets: • 90% of all people living with HIV will know their HIV status. • 90% of all people with diagnosed HIV infection will receive sustained antiretroviral therapy. • 90% of all people receiving antiretroviral therapy will have viral suppression. • Prevention targets 2020: • 90% awareness (face to face, interactive media – KP, YP) • 90% empowerment (young women, sex workers, MSM) • 90% service access (KP, condoms, PrEP) • 90% uptake (high impact interventions – condoms, VMMC, PrEP) Zero new HIV infections Zero Discrimination Zero AIDS-related deaths
HIV Response in South Sudan • Ratio of newly infected to initiated on treatment 4:1 (Africa avg ≈2:1); 20:1 ratio of new infections to ever enrolled on treatment • Less than 5% of PLHIV are on treatment (9% at CD4 count 350) • Only 20% of HIV positive pregnant women are able to access prevention of mother to child transmission services • MoH estimates 50,000 people test for HIV every year, we need to reach 700,000 a year to scale up treatment • About 10 million condoms are reported to be distributed annually, about 8% of what is required (110 million) to have an impact on new infections
National Strategic Plan 2013 - 2017 1. Reduction of new HIV infections by 50% by 2017 3 Outcomes: Reduction of risky sexual behaviour; PMTCT; health care settings 2. Reduction of mortality among men, women and children living with HIV by 50% by 2017 3 Outcomes: ART increased to 80% (in both adults & children) by 2017; retention on HIV care and treatment; and access to safety nets and IGAs. Priority target groups: • key populations: sex workers & clients; mobile populations -truck drivers, traders & migrant workers; uniformed groups • populations of humanitarian concern : refugees, IDPs and returnees • young people (10 – 24 years). Priority regions and locations: • Greater Equitoriaregion – high prevalence and hotspots • North-western South Sudan – low prevalence, low knowledge/access to services
HIV-Humanitarian Strategy 2014 - 2016 • Provides a national framework for the provision of HIV prevention, treatment and care services to populations of humanitarian concern • Aims to build sustainable national capacity for HIV programming in emergency contexts • Seeks to foster stronger collaborative arrangements between HIV and humanitarian actors at national and local levels Three key actions for Education Cluster: • Conduct Behavioural Change Communication programmes whenever the operational context is conducive (linked to life skills program) • Conduct in-house and partner trainings on HIV mainstreaming • Establish and strengthen HIV in the Workplace programmes targeting all staff
IASC Guidelines: HIV in Education • Children and young people with access to education are also more likely to delay onset of sexual activity and avoid alcohol and substance abuse • Education can provide life-saving knowledge, skills and services to children and young people vulnerable to HIV infection • Education can provide additional protection for those already infected and affected • Education can help raise awareness in the larger community IASC Guidelines: http://www.humanitarianinfo.org - IASC Products: HIV/AIDS Also INEE Minimum Standards Toolkit: HIV/AIDS www.ineesite.org/uploads/documents/store/doc_1_INEE_toolkit_-_HIV-AIDS.pdf
HIV situation stemming from crisis ≈ 40,000 PLHIV affectedwith little to no access to treatment, care and support networks ≈ 25,000 PLHIV displaced and likely in urgent need of HIV treatment, care and support services ≈ 1,000PLHIVhave interrupted treatment Vulnerability factors: • Family separation – high risk sexual behaviors, especially among young men • GBV - rape, sexual exploitation, intimate partner violence • Negative coping mechanisms – transactional sex, sex work • Little knowledge of HIV and HIV prevention • Low access to HIV services and prevention commodities (condoms) • Displacement to higher HIV prevalence locations
HIV in humanitarian response • Tracing and referring clients on ART, CTX and TB treatment • Provision of HIV services in IDP sites: • Awareness/behavioral change communication – HIV, GBV • Condom promotion • HIV counseling and testing • Prevention of mother to child transmission • Mobile and referral for treatment • SRH and MNCH linkages, including PSS and PEP for GBV survivors, and STI management • Resource mobilisation – GFATM, Humanitarian?
Opportunity for integration: IEC materials for BCC Five sets developed and approved, in English and Arabic: • HIV Basic Information • HIV Counseling and Testing • Prevention of mother to child transmission • Stigma and Discrimination • Snakes and Ladders Game for young people For your own sets, contact Mango Tree: Mathias Mwene – Country Manager, MT South Sudan mmwene@mangotreeuganda.org Tel South Sudan: +211927221638 Uganda: +256 703 071 172 / +256 312 263 263 Cost: ≈ USD250 for all 5 sets HIV IEC materials developed for UN staff also available for work place programme
Mumtaz Mia – Program Adviser Email: miam@unaids.org Mobile: 0912 112 299 www.aidsandemergencies.org Omar Dia – Humanitarian Adviser Email: diao@unaids.org Mobile: 0912 154 719 www.unaids.org