Download
1 / 10
110 likes | 346 Views
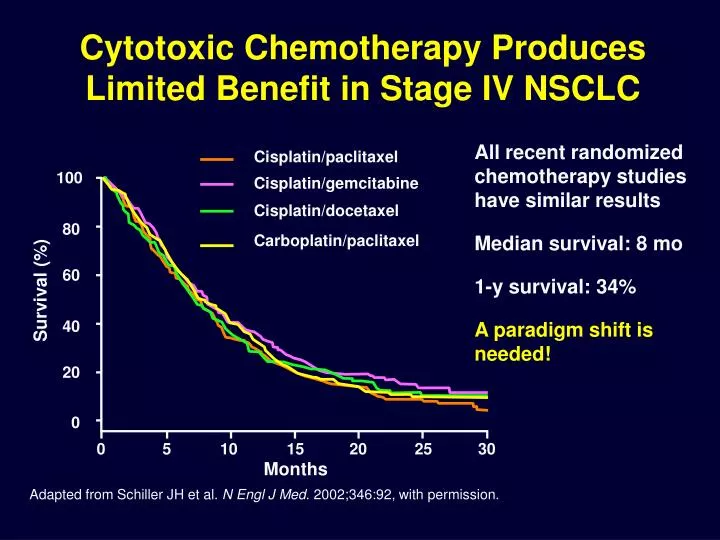
Cytotoxic Chemotherapy Produces Limited Benefit in Stage IV NSCLC. All recent randomized chemotherapy studies have similar results Median survival: 8 mo 1-y survival: 34% A paradigm shift is needed!. Cisplatin/paclitaxel. 100. Cisplatin/gemcitabine. Cisplatin/docetaxel. 80.

E N D
Cytotoxic Chemotherapy Produces Limited Benefit in Stage IV NSCLC All recent randomized chemotherapy studies have similar results Median survival: 8 mo 1-y survival: 34% A paradigm shift is needed! Cisplatin/paclitaxel 100 Cisplatin/gemcitabine Cisplatin/docetaxel 80 Carboplatin/paclitaxel 60 Survival (%) 40 20 0 0 5 10 15 20 25 30 Months Adapted from Schiller JH et al. N Engl J Med. 2002;346:92, with permission.
P P P P VEGFA Key Mediator of Angiogenesis Environmental factors (Hypoxia, pH) Growth factors Hormones (EGF, bFGF, PDGF, IGF-1, IL-1, IL-6, estrogen) Genes involved in tumorigenesis (p53, p73, src, ras, vHL, Scr-Abl) Increased VEGF levels Binding and activation of VEGFR Endothelial cell activation Survival Proliferation Migration ANGIOGENESIS VEGF = vascular endothelial growth factor; EGF = epidermal growth factor; bFGF = basic fibroblastic growth factor; PDGF = platelet-derived growth factor; IGF = insulin-like growth factor; IL = interleukin; VEGFR = VEGF receptor. Adapted from Gerber H-P, et al. Cancer Res. 2005;65:671, with permission from the American Association for Cancer Research.
rhuMAb VEGFBevacizumab • Humanized to avoid immunogenicity • 93% human, 7% murine • Recognizes all isoforms of VEGF, Kd = 1.1 nmol/L • Terminal t1/2 = 20 days • 1st phase I done at MDACC Gerber H-P, et al. Cancer Res. 2005;65:671.
Bevacizumab Phase III Study (E4599) Paclitaxel 200 mg/m2 + carboplatin AUC 6 mg/mL/min (PC) q3wk x 6 (unless progression or unacceptable toxicity) (No crossover permitted) 1st-line treatment of patients with stage IIIB with malignant pleural effusion,stage IV, or recurrent NSCLC (N = 878) Bevacizumab 15 mg/kg + PC q3wk (BV/PC) × 6 (unless progression or unacceptable toxicity) BV 15 mg/kg q3wk until progression or unacceptable toxicity Stratified by Disease stage Degree of weightloss Prior radiotherapy Measurable disease • Endpoints • Primary: Overall survival • Secondary: Response rates • Progression-free survival Toxicity Sandler A, et al. N Engl J Med. 2006;355:2542.
PC BV/PC Phase III Trial of Bevacizumab Overall Survival 100 80 Median 12.3 mo 60 Overall Survival (%) Median 10.3 mo 40 HR: 0.79, P = .003 20 0 12 24 36 0 6 18 30 42 48 Month PC = paclitaxel/carboplatin; BV = bevacizumab; HR = hazard ratio. Adapted from Sandler A, et al. N Engl J Med. 2006;355:2442, with permission.
Phase III Trial of BevacizumabAdverse Events Patients (%) PC(n = 440) BV/PC(n = 427) Event Severe or fatal hemorrhage1,* 1.1 4.7 0.9 0.0 Gastrointestinal perforation1 Pulmonary hemorrhage1 0.5 2.3 Arterial thrombotic events1 1.4 3.0 Hypertension (grade 3 or 4)2 0.7 7.0 Febrile neutropenia2 2.0 5.2 Severe proteinuria2 0.0 3.0 *Some events are reported as >1 site. PC = paclitaxel; BV = bevacizumab. 1. Avastin(bevacizumab). Product Information. San Francisco, CA: Genentech; 2006. 2. Sandler A, et al. N Engl J Med. 2006;355:2542.
Rationale for Combination Targeted Therapy for Advanced NSCLC bFGF = basic fibroblast growth factor; TGF- = transforming growth factor alpha. Herbst RS, et al. J Clin Oncol. 2005;23:2544. Reprinted with permission from the American Society of Clinical Oncology.
Bevacizumab Combination RegimensEfficacy and Safety Summary Chemotherapy Bevacizumab + Bevacizumab + Alone (n = 41) Chemo (n = 40) Erlotinib (n = 39) Progression-free survival Median, months 3.0 4.8 4.4 Adjusted hazard ratio* (95% Cl) NA 0.66 (0.38, 1.16) 0.72 (0.42, 1.23) Overall survival 6-month rate, % 62.4 72.1 78.3 Response rate, n (%) CR.PR 5 (12.2) 5 (12.5) 7 (17.9) CR/PR/SD 16 (39.0) 21 (52.5) 20 (51.3) EFFICACY SUMMARY *Adjusted by randomization stratification factors (ECOG PS, smoking history) Chemotherapy Bevacizumab + Bevacizumab + Alone (n = 41) Chemo (n = 40) Erlotinib (n = 39) Drug discontinuation due to AE, n (%) 10 (24) 10 (25) 4 (10) SAEs, n (%) 22 (54) 16 (40) 13 (33) Grade 5 drug-related AEs 2 (5) 3 (8) 1 (3) Pulmonary hemorrhage (grade 3–5) 0 2 (5) 1 (3) SAFETY SUMMARY Fehrenbacher L, et al. 42nd ASCO; June 2-6, 2006. Abstract 7062. Courtesy of Dr. L. Fehrenbacher.
Ongoing Randomized Studies with Bevacizumab/Erlotinib Combined Atlas (1st-line)1 Arm 1: bevacizumab + placebo to PD 1st-linestage IIIb/IVNSCLC(N = 1150) RANDOMIZE(Patients w/o PDor sig. toxicity) Chemotherapy + bevacizumab x 4 Arm 2: bevacizumab + erlotinib to PD Beta (2nd-line)2 Arm 1: erlotinib + placebo to PD 2nd-lineNSCLC(N = 650) RANDOMIZE Arm 2: erlotinib +bevacizumab to PD PD = progressive disease. 1. http://clinicaltrials.gov/ct/show/NCT00257608?order=1. 2. http://clinicaltrials.gov/ct/show/NCT00130728?order=8.
Characteristics of VEGFR TKIs New agent, BIBF 1120 reported to be a triple angiokinase inhibitor that targets VEGF, FGF, and PDGF receptors. *Biochemical IC50 values were determined using slightly different methods between the studies and are not directly comparable. 1. Mendel DB, et al. Clin Cancer Res. 2003;9:327. 2. Wilhelm SM, et al. Cancer Res. 2004;64:7099. 3. www.rxlist.com/cgi/generic/nexavar_cp.htm. 4. Wedge SR, et al. Cancer Res. 2005;65:4389. 5. Polverino A, et al. Cancer Res. 2006;66:8715. 6. Wedge SR, et al. Cancer Res. 2002;62:4645. 7. Rugo HS, et al. J Clin Oncol. 2005;23:5474. 8. Morabito A, et al. Oncologist. 2006;11:753. 9. Hess-Stumpp H, et al. ChemBioChem. 2005;6:550.