Download
1 / 17
440 likes | 1.44k Views
Peripheral Neuropathy (PN) or Chemotherapy-Induced Peripheral Neuropathy (CIPN). Objectives. The learner will be able to: Describe the pathophysiology of the various types of CIPN. Identify assessment strategies for PN/CIPN. Definition.

E N D
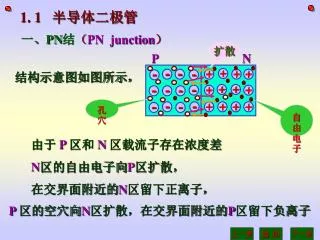
Peripheral Neuropathy (PN)orChemotherapy-Induced Peripheral Neuropathy (CIPN)
Objectives The learner will be able to: • Describe the pathophysiology of the various types of CIPN. • Identify assessment strategies for PN/CIPN.
Definition • Often thought to refer only to numbness and tingling of the hands or feet • PN is a group of neurologic dysfunctions that occur outside the spine and brain. • Refers to any part of the body affected by peripheral nerves
Incidence In those receiving neurotoxic chemotherapeutic agents, the incidence of developing PN can range from 10% to 100%.
Risk Factors Comorbidities: • Diabetes • Alcohol overuse • Metabolic imbalances • Vitamin B12 deficiency • Cachexia • HIV • Other paraneoplastic syndrome • Cancer • Age • Medications
Pathophysiology • CIPN is not understood totally. • Can vary depending on the type of chemotherapy given • Chemotherapy is believed to damage the sensory axons first and then cause degeneration and dying of axons and myelin sheaths.
Pathophysiology • Axons can regenerate if the offending agent is removed. • Damage to cell bodies is often not completely reversible.
Characteristics Sensory CIPN: • Negative manifestations such as numbness or reduced sensation • Positive symptoms/pain sensations such as paresthesia, dysesthesia, causalgia, and allodynia • Large sensory nerve damage may result in decreased deep tendon reflexes and vibratory sense, ataxia, and abnormal position sense of body parts.
Characteristics • Motor CIPN and autonomic CIPN are uncommon. • Motor CIPN is difficult to characterize as it is related to sensory damage, such as weakness, loss of feeling, or foot pain. • Autonomic CIPN can cause nausea, abdominal fullness or bloating, early satiety, constipation, urinary issues, and erectile dysfunction.
Associated Chemotherapy • Vinca alkaloids, taxanes, and platinum analogs are most commonly implicated—Dose-limiting CIPN • Less commonly, high-dose ifosfamide, high-dose methotrexate, etoposide, procarbazine, cytarabine, suramin, bortezomib, thalidomide, and arsenic trioxide • CIPN may occur during or soon after chemotherapy administration. • CIPN may progress with increasing doses or worsen after some drugs have been discontinued.
Assessment • Grading tools are available to grade the toxicity. • Determine the level of functional impairment. • Focus on evaluating from the patient’s perspective (subjective data).
Assessment Tools • Semmes-Weinstein filaments for cutaneous touch • Vibration—Nerve conduction • Reflexes • Assessment of temperature • Proprioception—Romberg test for balance • Sharp/dull sensation—Pinprick test • Gait assessment—Walking on heels and toes • Muscle strength—From no contraction to active movement against full resistance • Patient-reported symptoms
Medical Management of CIPN • Accurate assessment is essential! • Dose adjustment of chemotherapy • Pharmacologic interventions (effectiveness not yet established) • IV or oral calcium/magnesium • Glutathione • Supplemental vitamin E • Amifostine, glutamate, and glutamine • Xaliproden
Painful CIPN Agents to decrease dysethetic pain: • Anticonvulsants • Tricyclic antidepressants • Opioids • Topical agents
Patient Teaching • Self-report measures • Identify triggers • Self-care measures • Online educational sites
Nursing Considerations • Complex causes with few treatments • Goals should consider quality of life. • Nurses are an integral part of the team to help manage CIPN, especially with ongoing assessment.
References Biedrzycki, B.A. (2010). Peripheral neuropathy. In C.G. Brown (Ed.), A guide to oncology symptom management (pp. 405421). Pittsburgh, PA: Oncology Nursing Society. Oncology Nursing Society. (2009). Putting evidence into practice: Peripheral neuropathy. Retrieved from http://www.ons.org/Research/PEP/Peripheral Wickham, R. (2007). Chemotherapy-induced peripheral neuropathy: A review and implications for oncology nursing practice. Clinical Journal of Oncology Nursing, 11, 361376.