Download
1 / 29
290 likes | 398 Views
Clinical Use of Blood Components. Salwa Hindawi Director of Blood Transfusion Services KAUH, Jeddah KSA SITMS 24 th March 2004. Donor Patient. The risks associated with transfusion can be reduced by: - Effective blood donor selection.

E N D
Clinical Use of Blood Components Salwa Hindawi Director of Blood Transfusion Services KAUH, Jeddah KSA SITMS 24th March 2004
Donor Patient The risks associated with transfusion can be reduced by: - Effective blood donor selection. - Screening for TTI in the blood donor population. high quality blood grouping, compatibility testing. - Component separation and storage. - Appropriate clinical use of blood and blood products. - Quality assurance
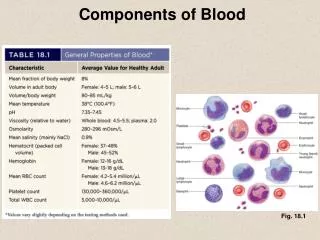
Blood Products Any therapeutic substance prepared from human blood: Whole blood 1-Blood components Red Cell Concentrate and suspension Platelet Concentrate Plasma – FFP Cryoprecipitate Cryosupernatent
2- Plasma Derivatives Human plasma proteins prepared from plasma under Pharmaceutical Manufacturing Conditions • Albumin • Coagulation factors concentrates • Immunoglobulins
Principles of Clinical Transfusion Practices • Avoid blood transfusion • Transfusion is only one part of the patient’s management. • Prevention and early diagnosis and treatment of Anemia & underlying condition • Use of alternative to transfusion. eg. IV fluids • Good anesthetic and surgical management to minimized blood loss.
* Prescribing should be based on national guidelines on the clinical use of blood taking individual patient needs into account. * Hb level should not be the sole deciding Factor Clinical evaluation is important
* The clinician should record the reason for transfusion clearly. * A trained person should monitor the transfused patient and if any adverse effects occur respond immediately.
WHEN WE SHOULD TRANSFUSE BLOOD ?&WHAT BLOOD COMPONENT SHOULD BE TRANSFUSED ?
Unnecessary transfusion can: • Expose the patient to unnecessary risks • Cause a shortage of blood products for patients in real need. Blood is an expensive, scarce resource.
Triggers of Component Transfusion • The lowest threshold for transfusion of components are: • Hb level of 6-7g/dl. Clinical judgment • FFP threshold PT & PTT 1.5 times the upper limit of the normal range. • Platelet threshold of: 10 000/µl- 20 000/µl for prophylactic transfusion
Invasive or surgical procedures: • 20 000/µl for BMA and Biopsy • 50 000/µl for surgery, massive transfusion, Liver cirrhosis. 100 000/µl for surgery to brain or eye. American Society of clinical Oncology guidline,1996&2001. Williamson LM. Transfusion Trigger in the UK. Vox sang 2002. AABB Technical Manual 14th ed, 2002.
Evidence based medicine through randomized controled trials and or clinical practice The use of a 7g/dl Hb threshold in critical care patients with maintenance of Hb of 7-9g/dl resulted in a 54%decrease in the number of transfused red cells and decrease exposure to any red cell by 33%. Hebert ,et al. N Engl J Med 1999
255 patients with acute myeloid leukemia Evaluated prospectively: • 135 patients were assigned to 10 000/mm3 threshold group • 120 were assigned to 20 000/mm3 • The risk of major bleeding was similar • Platelet use reduced by 21.5% in the lower threshold group Rebulla et al.N Engl J Med 1997.
The Appropriate Use of Blood and Blood Products • Safe Product (Supply safe accessible at reasonable cost, adequate) • Weight the risk against benefit
ALTERNATIVES TO BLOOD TRANSFUSION • CRYSTALLOID SOLUTIONS • COLLOID SLOUTIONS • DRUGS • BLOOD SUBSTITUTES
Guidelines on: • Ordering Blood • Indications • Compatibility policy differ from center to another • Collecting blood products prior to transfusion • Administration • Monitoring the transfusion • Adverse effect of transfusion
Transfusion committee • Surgery • Infection Control • Transfusion specialist or Haematologist • Pediatrics • Obstetrics • Anesthesia • Medicine • Nurse • QA
The committee shall be responsible for: • Developing the guidelines for transfusion • Reviewing of the use of blood and its components • Reviewing structure, process , outcomes and utilization Indicators.
Reviewing all reports regarding transfusion reaction & Incident reports • Promote education and training of all clinical and support Staff involved in blood transfusion. • Have the authority to modify and implement the existing Blood transfusion protocols
Maximum Surgical Blood Ordering Schedule (MSOS) • MSOS is a table of elective surgical procedures that lists the number of units of blood routinely cross-matched pre-operative. • The ideal value for cross matched to transfused blood, C:T ratio is 1:1 . • An acceptable value is 3:1 - 2:1 which corresponds to a blood usage of 30-50%.
A checklist for cliniciansAlways ask yourself the following questions before prescribing blood or blood products for a patient • What improvement in the patient's clinical condition am I aiming to achieve? • Can I minimize blood loss to reduce this patient's need for transfusion • Are there any other treatments I should give before making the decision to transfuse, such as intravenous replacement fluids or oxygen?
What are the specific clinical or laboratory indications for transfusion for this patient? • What are the risks of transmitting HIV, hepatitis, syphilis or other • Infectious agents through the blood products that are available
What other options are there if no blood is available in time? • Will a trained person monitor this patient and respond immediately if any acute transfusion reactions occur? • Have I recorded my decision and reasons for transfusion on the patient's chart and the blood request form?
Finally, if in doubt, ask yourself the following question. • If this blood was for myself or my child, would I accept the transfusion in these circumstances?
Conclusions 1 • Availability of safe blood Evidence-based clinical guidelines for usage of blood &blood products. • Correct management of blood inventory to prevent blood units wastage & outdating. • Promotion of blood component therapy.
Conclusions2 • Hospital transfusion committee. • Training & education for laboratory staff , students & treating physician. • Availability and accessibility of blood substitutes. • Auditing
References • The Clinical use of Blood Handbook, WHO Blood Transfusion safety, Geneva • AABB technical Manual 14th Edition 2002. • Handbook of transfusion Medicine 3rd edition