Download
1 / 10
100 likes | 195 Views
QIPP initiative analysis: summary by PCT by type – shown cumulatively for impact on gap. QIPP initiative analysis: detail by PCT by year. Cumulative impact of initiatives on cumulative gap. Cumulative impact of initiatives on cumulative gap. In £m’s. Menu of improvement opportunities.

E N D
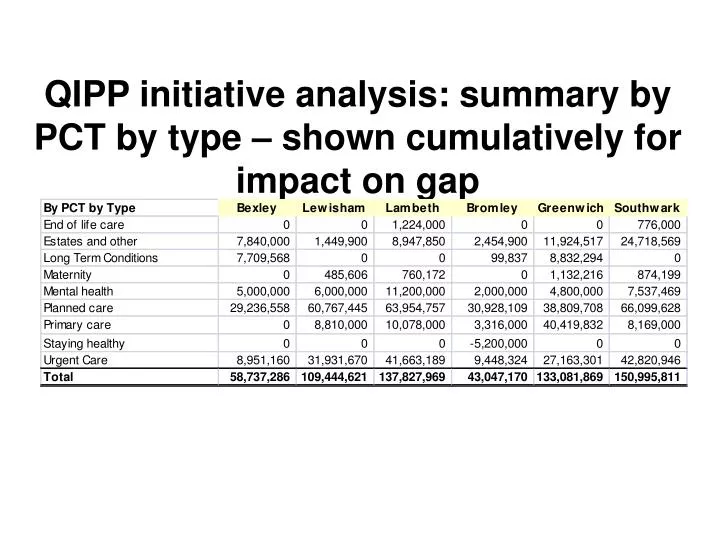
QIPP initiative analysis: summary by PCT by type – shown cumulatively for impact on gap
Menu of improvement opportunities Initiative: Right Care, Right Place Focus: Reconfiguration of local secondary services in as part of shift to polysystems (e.g. outpatients and diagnostics) Redesign of certain planned and LTC pathways (e.g. diabetes, COPD, MSK, sexual health, end of life and dementia) Decommission and/or introduce evidence based thresholds for PoLCE Primary care management of out patient referrals Rationale: Currently no structured or integrated care for COPD and adult asthma patients Improve the diabetes care pathway and ensuring delivery of a greater part of the pathway in the community. Expand the current model of service and use the Long Term Conditions models for delivering a Heart Failure service in the community. Establish Referral Management Centres as part of a package of measures to address referral management Outcomes: Savings will be achieved by decommissioning – in year 1 and 2, with patients actively discharged to primary care. Implementation of LTC Development Programme will raise the standard of primary care to achieve Tier 1 services. From year 3, savings will be achieved by continued primary care management and shift to community based walk-in multi-disciplinary clinics. Target to shift 80% of OP activity to community settings
Menu of improvement opportunities Initiative: Specialist services Focus: KCH is accredited as a HASU and Major Trauma Centre GSTT has the Dimbleby Cancer centre Vascular inpatient services across KCH and GSTT are to be centralized onto one site Rationale: Improve access to cancer services Improve secondary prevention for cardiac and vascular diseases. Prevention and improved management of stroke and heart disease Outcomes: Decentralizing some of the ambulatory specialist services (inc. chemotherapy) across SEL Centralising of specialist services e.g. aspects of cardiac Centralise the number of paediatric inpatient units Reductions in hospital admissions Improved quality of services to those who are at the end of their lives
Menu of improvement opportunities Initiative: Cancer Focus: Implement the CSL Cancer model of care Rationale: Overseeing enhanced recovery after surgery (ERAS) in all acute trusts in a range of tumour sites. Meeting the 14 day turnaround from the cervical screening test to receipt Implementing the acute oncology measures for all trusts with an A&E Commissioning new models of care for systemic therapy services Implementation of revised tariff and recharge mechanisms for commissioning of systemic therapy services Outcomes: ERAS 14 day Turnaround Establishment of an acute oncology service in all hospitals with an A&E Systemic therapy
Menu of improvement opportunities Initiative: Urgent Care The focus of this initiative is: Development of Urgent Care Centres Diversion to primary care for primary care interventions Rationale: Build on the success of the rapid response team Single point of telephone access to urgent care Providing greater clarity for local people on how to access these services. Outcomes: Reduced inappropriate use of A&E Better management of primary care conditions in primary care Increase the number of terminally ill cancer and non cancer patients enabled to die in their own home.
Menu of improvement opportunities Initiative: Medicines management Focus: Drugs related savings Maximising the scope for further in year savings on drugs. New contract monitoring processes for high cost drugs Rationale: The growth rate in 2009/10 for primary care prescribing was 2.9% Increase for 2010/11 on 2009/10 spend was 1% Current forecast is £1million overspend on primary care prescribing budget of £35million. Outcomes: Reductions in spend achieved by: Procurement Clinical effectiveness/VFM Leverage increased buying power of purchasing consortia / more effective procurement of clinically effective drugs Enforce compliance for drugs for OP prescriptions Ensure drugs are used within guidelines Increased use of generics and reduced variability on prescribing