Download
1 / 26
270 likes | 411 Views
Hospital Acquired Conditions Use of Oxidative Technology. Surface Recharge You Clean and Disinfect, but it Keeps Coming Back. Hospital Acquired Conditions HACs.

E N D
Hospital Acquired Conditions Use of Oxidative Technology Surface Recharge You Clean and Disinfect, but it Keeps Coming Back
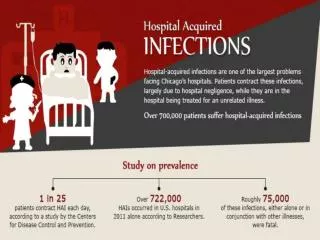
Hospital Acquired Conditions HACs The microorganisms that cause nosocomial infections have been well cataloged and the infections they cause are fairly well understood, but the traditional solutions, cleaning, scrubbing, disinfectants, ventilation, filtration, management and procedural controls, etc., have failed to completely eliminate the problem. Kowalski, Wladyslaw. Hospital Airborne Infection Control. CRC Press, 12/2011. What is going on in the air?
HACs Surgical Site Infections are often the most problematic and fatal type infection that can occur in hospital settings. Many SSIs are thought to be transmitted only by direct contact, either hand to patient or hand to equipment, or equipment to patient, but this view over looks the fact that both hands and equipment may pick up contamination from elsewhere, and that may include settling from the air. Once settled, they may be resuspended by activity. Although direct contact is regarded as being the primary mode of contamination of surgical sites, airborne transmission can occur. Mangram etal. 1999 Breaking the Cycle
Legislation Section 5001(c) of Deficit Reduction Act of 2005 requires the Secretary to identify conditions that are: (a) high cost or high volume or both, (b) result in the assignment of a case to a DRG that has a higher payment when present as a secondary diagnosis, and (c) could reasonably have been prevented through the application of evidence‑based guidelines. On July 31, 2008, in the Inpatient Prospective Payment System (IPPS) Fiscal Year (FY) 2009 Final Rule, CMS included 10 categories of conditions that were selected for the HAC payment provision. Payment implications began October 1, 2008, for these Hospital Acquired Conditions. http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalAcqCond/Hospital-Acquired_Conditions.html The Affordable Care Act of 2010 established the Hospital VBP Program, which applies to payments beginning in Fiscal Year (FY) 2013, on or after October 1, 2012, and affects payment for inpatient stays in 2,985 hospitals across the country.
What CMS is doing: Since October 1, 2007, hospitals have been required to report on their Medicare claims if any of the first eight selected conditions were present at the time the patient was admitted to the hospital, and beginning October 1, 2008, will have to report on the remaining conditions as well. If at discharge, there is a selected condition that was either not identified by the hospital as present on admission, or could not be identified based on data and clinical judgment at admission, it is considered hospital-acquired. To encourage hospitals to avoid hospital-acquired conditions, beginning October 1, 2008, Medicare will no longer pay hospitals at a higher rate for the increased costs of care that result when a patient is harmed by one of the listed conditions if it was hospital-acquired. Medicare prohibits the hospital from billing the beneficiary for the difference between the lower and higher payment rates. Medicare will pay for physician and other covered items or services that are needed to treat the hospital-acquired condition, including the costs of post-acute care that would not have been needed for the patient’s initial medical problem, but are needed because of the hospital-acquired condition. http://www.cms.gov/apps/media/press/factsheet.asp The Hospital Value-Based Purchasing (VBP) Program is a Centers for Medicare & Medicaid Services (CMS) initiative that rewards acute-care hospitals with incentive payments for the quality of care they provide to people with Medicare. The Affordable Care Act of 2010 established the Hospital VBP Program, which applies to payments beginning in Fiscal Year (FY) 2013, on or after October 1, 2012, and affects payment for inpatient stays in 2,985 hospitals across the country Facts
Average cost of a Healthcare Acquired Condition in the US, the annual economic impact of HAIs was approximately $6.5 billion in 2004 . Recently Zimlichman and colleagues conducted a systematic review of the literature for the years 1986 through 2013 for an updated estimate of costs associated with the most significant and targetable HAIs in the US. These were CLABSI, VAP, SSI, CR-UTI, and C. difficile infection (CDI). On a pair case basis, CLABSI were found to be the most costly at $45,814 (95% CI, $30,919-$65,245), followed by VAP at $40,144 (95% CI,$36,286-$44,220), SSI at $20,785 (95% CI, $18,902-$22,667), CDI at $11,285 (95% CI, $9,118-$13,574), and CR-UTI at $896 (95% CI, $603-$1,189). Based on 2009 data where approximately 34.7 million adults received inpatient care in US hospitals (totaling 165 million patient days), the total annual cost of the 5 infections was $9.8 billion (95% CI, $ 8.3-11.5 billion) with SSI and CDI being the most frequent (36% and 30% respectively). Costs
CMS new “value” vs. old “fee-based” reimbursement DEPARTMENT OF HEALTH AND HUMAN SERVICES Centers for Medicare & Medicaid Services Hospital Value-Based Purchasing Program The Hospital Value-Based Purchasing (VBP) Program is a Centers for Medicare & Medicaid Services (CMS) initiative that rewards acute-care hospitals with incentive payments for the quality of care they provide to people with Medicare. How Does Hospital Value-Based Purchasing Work? CMS rewards hospitals based on the quality of care provided to Medicare patients, how closely best clinical practices are followed, and how well hospitals enhance patients’ experiences of care during hospital stays. Hospitals are no longer paid solely based on the quantity of services they provide. The Affordable Care Act of 2010 established the Hospital VBP Program, which applies to payments beginning in Fiscal Year (FY) 2013, on or after October 1, 2012, and affects payment for inpatient stays in 2,985 hospitals across the country. Under the Hospital VBP Program, Medicare makes incentive payments to hospitals based on either: 1) How well they perform on each measure, or 2) How much they improve their performance on each measure compared to their performance during a baseline period. “Changing the way we pay hospitals will improve the quality of care for seniors and save money. Under this initiative, Medicare will reward hospitals that provide high quality care and keep their patients healthy. It’s an important part of our work to improve the health of our nation and drive down costs.” Kathleen Sebelius, Secretary of the U.S. Department of Health and Human Services (HHS) April 29, 2011 ICN 907664 March 20132 Reimbursement Reducing HAC occurrences will impact “value” of care
Consider this: If we consider the fact that most fomite contamination of surfaces, especially horizontal surfaces like floors, must arrive via the air, then we must admit that airborne transport plays a role in surface contamination. Kowalski, Wladyslaw. Hospital Airborne Infection Control. CRC Press, 12/2011. Keeping Surfaces Clean Matters
Biological Air Cleaning – Settling Rates • Settling rates in still air • Turbulence from fans, people moving will increase settling times • <.1 micron particles stay suspended indefinitely Settling Rates Who Knew
Hospital Ventilation It is assumed that hospital ventilation systems are designed in accordance with appropriate guidelines and codes, and are not subject to internal mold growth and excessive condensation, and that they do not have outside air intakes too close to roof exhausts or cooling towers. Dilution Ventilation removes all airborne pathogens at approximately equal rates if complete mixing occurs, but some larger microbes and spores may settle out and remain on surfaces. Ventilation air may also add microbes from outdoor air if there is no filtration or filtration is inadequate. Filtration: Breakthrough Integrity of Design
HEPA filtration effectiveness has been examined to determine the most penetrating microorganisms. For a single pass through a HEPA 99.97% filter, the number of penetrations per million for each microbe in Table 1 was calculated. Figure 9 shows the results of this analysis, where only those microbes that experienced penetration above about 30 per million are listed. All of the microbes between H. influenzae and Varicella experienced penetrations greater than 1 in 10,000. This may be insignificant, especially for a single pass through the filter, but it depends on the airborne concentration and the infective dose for each microorganism. The infective dose for M. tuberculosis is 1-10 bacilli. An intriguing aspect of Figure 9 is that almost all of the most penetrating microorganisms are agents of nosocomial infections. ASHRAE Transactions: Research Filtration of Airborne Microorganisms: Modeling and Prediction W.J. Kowalski, M.S., P.E. William P. Bahnfleth, Ph.D., P.E. T. S. Whittam, Ph.D. We have HEPA Filtration, we are following code?
ASHRAE Position Paper, June, 2009 What’s changed? Acknowledges that HVAC systems play a role in the dissemination of diseases in buildings. Key points: Infectious diseases can be transmitted via an airborne path Designers have a responsibility to minimize that potential • Dilution ventilation • Building pressure control • Filtration • Oxidative technologies, • UVGI, PCO
Reactive Oxygen SpeciesKnow the difference ACTIVE TECHNOLOGIES PASSIVE TECHNOLOGY Ionization: Broadcast ions creating hydroxyl radicals Photo Catalytic Oxidation: Creates hydroxyl s in the occupied breathing space. Bi-polar ionization: Broadcast ions creating hydroxyl radicals in the occupied breathing space. Photohydroionization: Broadcast hydrogen peroxide into the occupied breathing space. Ozone generators: Broadcast ozone into the occupied breathing space. PASSIVE TECHNOLOGY Photo Catalytic Oxidation: Creates hydroxyl radicals in a contained location, does not broadcast into occupied breathing space.
Using Passive Reactive Oxygen Species to destroy contaminants Like the atmosphere, Genesis works apart from where living creatures breathe Total Contaminants Various Sources Fresh Air Genesis Panel Kill Zone Treated Air Exhaled Breath Off Walls Invisible Airborne contaminants Significantly reduced viruses, mold, bacteria & TVOC’s Floors & Furnishings Working away from the occupied space: Passive Safe
Chamber Testing Testing performed by RTI International Validation Clean Air Delivery Rate (CADR) is a figure of merit that is the cubic feet per minute (CFM) of air that has had all the particles of a given size distribution removed. CADR rating were developed by the Association of Home Appliance Manufactures (AHAM) and are measured according to a procedure specified by ANSI/AHAM AC-1. The CDRm numbers in the graph are based off microbiologic Genesis Panels have been challenge with TB, Anthrax, Bacteria, Staph, E Coli, endotoxins, mycotoxins, viruses and VOCs.
Single Pass Testing performed by RTI International Validation There were no pre-filters this test and there was no recirculation of the air. These results reflect the efficacy of the Genesis Air PCP Standard panel alone in a single pass at a standard HVAC air speed • 1. Genesis Air PCO units either as standalone or in AHUs reduce the levels of CFUs in the air stream and a space. • 2. Genesis Air units in a single pass application at a removal rate of 99.9% for MRSA and 88.7% for Tuberculosis are a must for areas where high CFU levels would lead to higher infection and mortality rates from TB, MRSA and other nosocomial infections. • 3. In either single pass or in recirculating systems Genesis Air equipment alone (without filtration) will reduce bio-aerosol microbial contaminants. Genesis Panels have been challenge with TB, Anthrax, Bacteria, Staph, E Coli, endotoxins, mycotoxins, viruses and VOCs.
Genesis Panels as tested in the field slow surface recontamination Surface Testing
Surface Testing • Day 2 • Mark off 6x6 area on wall with wax pen • Hang sign for maintenance to not clean area • Swab surface in the 3” center of the square with Healthlink Transporter • After sample was taken the area was cleaned with Wexcide as per instructions from manufacture • Genesis Air Off being serviced
Surface Testing • Day 2 • Swab area • No surface cleaning took place • Genesis Air Off
Surface Testing • Day 6 • Swab sample area • Clean surface with Wexcide as per manufacture instructions • Turn Genesis Air system on
Surface Testing • Day 7 • Swab sample area • 7 total areas were sampled • No viable bacteria was found in the surface testing area after Genesis Air Panels were turned on.
Curb Mounted RTU New Construction or Retrofit in Curb Adaptor During your unit change outs why not improve your air quality.
2008 CU Inline or plenum mounted: Scalable fits all sizes of split systems Both horizontal & vertical
Recirculating for Individual Spaces Self-Contained IAQ Solution out of sight & out of mind. Inlet Ducted Attached to Filter grilles Mounted Above the Ceiling Supply Out 2008 DT FP
2006 D & L Small spaces wall mount or desktop