Download
1 / 128
1.29k likes | 1.35k Views
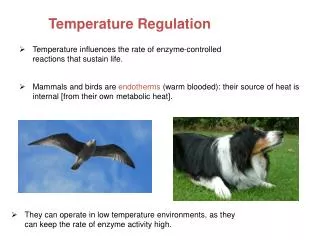
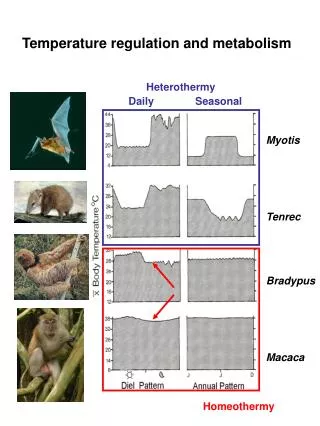
Temperature regulation and monitoring. Mammals and birds are homeothermic They require a nearly constant internal body temperature

E N D
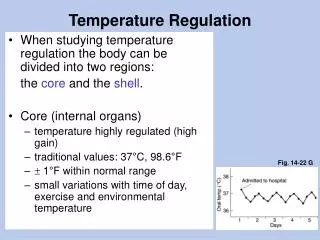
Mammals and birds are homeothermic • They require a nearly constant internal body temperature • When internal temperature deviate significantly from normal : metabolic functions deteriorate death • Thermoregulatory system maintainscore body temperature within 0.2 C of normal (37) • /.Anesthetic induced inhibition of thermoregulation /.cold operating room /.unwarmed patiients Hypothermic
Mild hypothermia1-2 C • Triples(3) morbid cardiac outcom • Triples(3) surgical wound infection • Prolongesrecovery time -hospitalization • Increases surgical blood loss and the need for allogeneic transfusion by about 20%
Normal thermoregulation • Afferent thermal sensing(input) • Central regulation • Efferent response
Afferent input • Cold-sensitivecells are anatomicallyand physiologically distinct from those that detectwarmth • Cold: A delta nerve fibers warm: unmyelinated C fibers (pain)
Most ascending thermal information traverses the spinothalamic tracts in the anterior spinal cord, but no single spinal tract is critical for conveying thermal information. • Consequently, the entire anterior cord must be destroyed to ablate thermoregulatory responses.
1/Hypothalamus 20%total thermal input 2/Other parts of brain to the3/Spinal cord (ant) central regulatory system4/Deep abdominal and thoracic tissues 5/Skin surface
Central control • Temperature is regulated by central structures (primarily the hypothalamus) that compare integratd thermal inputs from the skin surface, neuraxis, and deep tissues with thresholdtemperatures for each thermoregulatory response. • Most thermal information is "preprocessed" in the spinal cord and other parts of the central nervous system.
The slope of response intensity versus core temperature defines the gainof a thermoregulatory response. • This system of thresholds and gains is a model for a thermoregulatory system that is further complicated by interactions between other regulatory responses (i.e., vascular volume control) and time-dependent effects.
How the body determines absolute threshold temperatures isunknown, but the mechanism appears to be mediated by norepinephrine,dopamine, S-hydroxytryptamine, acetylcholine, prostaglandin E" and neuropeptides.
Thresholds vary daily in both sexes (circadian rhythm) and monthly in women by approximately 0.5°C. Exercise, foodintake, infection, hypothyroidism and hyperthyroidism, anesthetic and other drugs (including alcohol, sedatives, and nicotine), and cold and warm adaptationalter threshold temperatures.
Control of autonomic responses is approximately 80% determined by thermal input from core structures (Fig) In contrast, a large fraction of the input controlling behavioral responses is derived from the skin.
The interthreshold range(core temperatures not triggering autonomic thermoregulatory responses) is only 0.2°C. This range is bounded by the sweating threshold at its upper end and by vasoconstriction at the lower end.
Both sweating and vasoconstriction thresholds are 0.3°C to 0.5C higher in women than men, even during the follicular phase of the monthly cycle (first 10 days). Differences are even greater during the luteal phase.
Central thermoregulatory control is apparently intact even in somewhat premature infants. • In contrast, thermoregulatory control is sometimes impaired in the elderly."
Efferent responses • The body responds to thermal perturbations(body temperatures differingfrom the appropriate threshold) by activatingeffector mechanisms that increase metabolic heat production or alter environmental heat loss.
Each thermoregulatory effector has its own threshold and gain, so there is an orderly progression of responses and response intensities in proportion to need.
In general, energy-efficient effectors such as vasoconstriction are maximized before metabolically costly responses such as shivering are initiated.
Effectors determine the ambient temperature range that the body will tolerate while maintaining a normal core temperature.
When specific effector mechanisms are inhibited (e.g., shivering prevented by the administration ofmuscle relaxants), the tolerable range is decreased. Still, temperature will remain normal unless other effectors can not compensate for the imposed stress. • ,behavioralregulation(e.g., dressing appropriately, modifying the environmental temperature, assuming positions that oppose skin surfaces and voluntary movement) is themost important effector mechanism.
Infants regulate their temperatures remarkably well. In contrast, advanced age, infirmity, or medications can diminish the efficacy of thermoregulatory responses & increase the risk of hypothermia. • Mr: min tolarable ambient temperature (inhibit shivering) • Anticholinergics: max tolarable teper… (inhibit sweating)
Cutaneous vasoconstriction is the most consistently used autonomic effector mechanism. Metabolic heat is lost primarily through convection and radiation from the skin surface, and vasoconstriction reduces this loss. • Total digital skin blood flow is divided into nutritional(mostly capillary) and thermoregulatory(mostly arteriovenous shunt) components. • The arteriovenous shunts are anatomically and functionally distinct from the capillaries supplying nutritional blood to the skin (thus vasoconstriction does not compromise the needs of peripheral tissues).
Control of blood flow through arteriovenous shunts tends to be "on" or "off.“ • In other words, the gain of this response is high. • Local alfa-adrenergic sympathetic nerves mediate constriction in the thermoregulatory arteriovenous shunts, and flow is minimally affected by circulating catecholamines. • 10% of cardiac output traverses arteriovenous shunts; consequently, shunt vasoconstriction increases mean arterial pressure approximately 15 mm Hg.
Nonshivering thermogenesis increases metabolic heat production without producing mechanical work. • It doubles heat production in infants but increases it only slightly in adults.
Skeletal muscle and brown fat tissue are the major sources of nonshivering heat in adults. • The metabolic rate in both tissues is controlled primarily by norepinephrine release from adrenergic nerve terminals and is further mediated locally by an uncoupling protein.
Sustained shivering augments metabolic heat production 50% to 100% in adults. This increase is small in comparison to that produced by exercise (which can, at least briefly, increase metabolism 500%)and is thus surprisingly ineffective. • Shivering does not occur in newborn infants and is probably not fully effective until children are several years old
Sweating is mediated by postganglionic cholinergic Nerves. It is thus an active process that is prevented by nerve block or atropine administration. • Sweating is the only mechanism by which the body can dissipate heat in an environment exceeding core temperature. fortunately, the process is remarkably effective, with 0.58 kcal of heat dissipated per gram of evaporated sweat.
Active vasodilation requires intact sweat gland function, so it is also largely inhibited by nerve blocks. • The threshold for active vasodilationis usually similar to the sweating threshold, but the gain may be less. maximum cutaneousvasodilation is generally delayed until core temperature is well above that provoking the maximum sweating intensity.
THERMOREGULATION DURING GENERAL ANESTHESIA
Behavioral regulation is not relevant during general anesthesia because patients are unconscious and frequently paralyzed. • All general anesthetics tested thus far markedlyimpair normal autonomic thermoregulatory control. • Anesthetic-induced impairment has a specific form: warmresponsethresholds are elevated slightly whereas coldresponsethresholds are markedly reduced.
the interthreshold range is increased from its normal values near 0.3°C to approximately 2°C to 4°c. • The gain and maximum intensity of some responses remain normal, whereas others are reduced by general anesthesia.
Response Thresholds • Propofol, alfentanil, and dexmedetomidine all produce a slight linear increase in the sweatingthreshold a marked linear decrease in the vasoconstriction and shivering thresholds. • Isoflurane and desflurane also slightly increase the sweating threshold; they decrease the cold-response thresholds nonlinearly.
the volatile anestheticsinhibitvasoconstriction and shivering (less than propofol does at low concentrations, but more than propofol does at typical anesthetic doses.) • In all cases (except during meperidineand nefopamadministration), vasoconstriction and shivering decrease synchronously and thus maintain their normal approximate 1°C difference..
The combination of increased sweating thresholds and reduced vasoconstriction thresholds increases the interthreshold range about20-fold, from its normal value near0.2°C to around 2°C to 4°C. Temperatures within this range do not trigger thermoregulatory defenses; patients are thuspoikilothermic within this temperaturerange.
Halothane, enflurane,and the combination of nitrous oxide and fentanyldecrease the vasoconstriction threshold 2°C to 4°C from its normal value near approximately 37°C. However, the effect of these drugs on sweating or shivering remains unknown. Cl0nidine synchronously decreases cold-response thresholds while slightly increasing the sweating threshold. • Nitrous oxide decreases the vasoconstriction and shivering thresholds less than equipotent concentrations of volatile anesthetics do.
The only sedative or anesthetic drug tested that minimally influences thermoregulatory control is midazolam. • Painful stimulation slightly increases vasoconstriction thresholds. • thresholds will be somewhat lower when surgical pain is prevented by simultaneous local or regional anesthesia.
Responses in Infants and theElderly • Thermoregulatory vasoconstriction is comparably impaired in infants, children, and adults given isoflurane or halothane (Fig. 40_4). • In contrast, the vasoconstriction threshold is about 1°C less in patients aged 60 to 80 years than in those between 30 and 50 years old (Fig. 40_5).
Thermoregulatory vasoconstriction is comparably impaired in infants, children, and adults given isoflurane or halothane .
the vasoconstriction threshold is about 1°C less in patients aged 60 to 80 years than in those between 30 and 50 years old
Nonshiveringthermogenesis does not occur in anesthetized aduIts, which is unsurprising because this response is not particularly important in unanesthetized adults. • In contrast to adult humans, nonshiveringthermogenesis is an important thermoregulatory response in animals and human infants. However, nonshiveringthermogenesis in animals is inhibited by volatile anesthetics and it fails to increase the metabolic rate in infants anesthetized with propofol.
Gain and Maximum Response Intensity • Both the gain and maximum intensity of sweating remain normal during isoflurane and enflurane anesthesia. • The gain of arteriovenous shunt vasoconstriction is reduced threefoldduring desflurane anesthesia ,even though the maximum vasoconstriction intensity remains normal.
Shivering is rare during surgical doses of general anesthesia, its threshold being roughly 1°C less than the vasoconstriction threshold. • (Vasoconstriction usually prevents additional hypothermia, so even unwarmed patients rarely become cold enough to shiver.) shivering can be induced by sufficient active cooling.
Gain and maximumshivering intensity remain normal during both meperidine and alfentanil administration • Gain also remains nearly intact during nitrous oxide administration, although maximum intensity is reduced. • Isofluranechanges the macroscopic pattern of shivering to such an extent that it is no longer possible to easily determine gain. The drug does, however, reduce maximum shivering intensity.
Sweating appears to be the thermoregulatory defense that is best preserved during anesthesia. • Not only is the threshold only slightlyincreased, but the gain and maximum intensity are also well preserved. • In contrast, the thresholds for vasoconstriction and shivering are markedlyreduced, and furthermore, these responses are less effective than normal even after beingactivated.