Download
1 / 58
580 likes | 736 Views
Multi-drug resistant tuberculosis (MDR-TB) as a global problem. Dr. Şeref Özkara, Assoc. Prof ozkaraseref@yahoo.com Atatürk Chest Diseases and Chest Surgery ER Hospital, Ankara, Turkey. Stop TB in lights, WHO Headquarters, Geneva, Switzerland. 1994-1996: 35 location/country.

E N D
Multi-drug resistant tuberculosis (MDR-TB) as a global problem Dr. Şeref Özkara, Assoc. Prof ozkaraseref@yahoo.com Atatürk Chest Diseases and Chest Surgery ER Hospital, Ankara, Turkey Stop TB in lights, WHO Headquarters, Geneva, Switzerland.
1994-1996: 35 location/country 1996-1999: 58 location/country 1999-2002: 77 location/country
WHO/IUATLD Global Project onAnti-TB Drug Resistance Surveillance • Method: Standard1: • A sample representing patients • Enough sample size. • Standardized data collection (new and previously treated cases) • With Quality Assured Laboratories • Supported by Supra-National Reference Laboratories • Target: To find the resistance rates to drugs HRES 1. Guidelines for surveillance of drug resistance in tuberculosis. Geneva. WHO, 2003
WHO/IUATLD Global Project onAnti-TB Drug Resistance Surveillance - 1 1994-1996, 35 location/country
20 Supra-national reference laboratories • Proficiency testing of DST is done each year with a panel of 30 clinical isolates
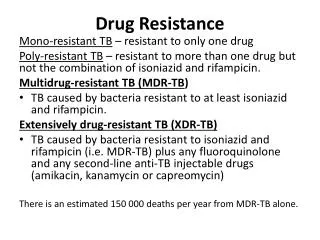
New terminology • Hot spots • Places with a high MDR-TB prevalence
MDR-TB, hot spots: Argentina, Dominician Republic, Estonia, Latvia, Ivory Coast, Ivanovo Oblast
WHO/IUATLD Global Project onAnti-TB Drug Resistance Surveillance – 2 1996-1999, 58 location/country
Terminology changed • Drug resistance in new cases • (previous term: “primary drug resistance”) • Drug resistance in previously treated cases • (previous terminology: “secondary drug resistance”) • “Hot spots” • MDR-TB prevalence 3% or more in new cases
MDR-TB prevelance in previously treated cases, median 9,1% (0%-42%)
First two reports: 1994-1999 • Drug resistance is present in all surveyed places • MDR-TB is present in many places • Places with a good TB control, drug resistance rates are low or decreasing
WHO/IUATLD Global Project onAnti-TB Drug Resistance Surveillance – 3 1999-2002, 77 location/country
Targets of the study • Recent profile of anti-TB drug resistance • Dynamics of resistance over time, trends • Major determinants of drug resistance • Evaluation of “hot spots” and how to define the burden of MDR-TB • Use of RİF resistance as a surrogate marker for MDR-TB • Evolution and amplification of resistance • Proficiency test results of laboratories over time
Drug resistance in new cases • 75 location, 55,779 patients • Any drug resistance: Some European countries 0%, Kazakhstan 57.1% (median 10.2%) • Median drug resistancei: SM, 6.3%; INH, 5.9%; RIF, 1.4%; EMB, 0.8% • MDR: eigh countries 0%, Kazakhstan ve Israel 14.2%, Median (1.1%) • Other high rates: • Tomsk Oblast (Russian F.) 13.7% • Karakalpakstan (Uzbekistan) 13.2% • Estonia 12.2% • Liaoning Provincei (China) 10.4% • Lituania 9.4% • Latvia 9.3% • Henan Province (China) 7.8% • Equator 6.6%
Drug resistance in previously treated cases • 66 location, 8,405 patients. • Median 18.4% drug resistance, Kazakhstan 82.1% • Median drug resistance, İNH, 14.4%; SM, 11.4%; RİF, 8.7%; EMB, 3.5% • Median MDR 7.0% • Highest MDR • Oman 58.3% • Kazakhstan 56.4% • Prevalence of drug resistance to 4 drugs • Previous Soviet Countries 30% • All other places 1.3%
MD-TB “hot spots” term • Cut-off point for MDR-TB “hot spots” is determined by statistical analysis as 6.6% and over.
Dynamics of drug resistance over time: New patients. Botswana, new cases, any drug resistance • Documented in 46 places • Resistance to any drug • INCREASE : Botswana, New Zealand, Polonia and Tomsk Oblast • DECREASE: cUBA, Hong Kong, Tailand • MDR-TB • INCREASE : Polonia and Tomsk Oblast • DECREASE: Hong Kong, Tailand, USA
Dynamics of drug resistance over time: Previously treted patients. • Documented 43 countries • Any drug resistance • INCREASE: Botswana • DECREASE: Cuba, Switzerland, USA • MDR-TB • INCREASE: Estonia, Lituania, Tomsk Oblast • DECREASE: Slovakia, USA Tomsk Oblast, MDR, all cases
Potential determinants of Drug Resistance • Bad or worsening TB control. • Patients immigrated from countries with high drug resistance rates • Differences in surveillance methods. -
Distribution of drug resistance (%) Highest in new cases : H, S, HS resistance Highest in previously treated cases: HRSE resistance
Use of RIF resistance as a surrogate marker for MDR-TB • RİF mono resistance, • Causes failures, important clinically and for public health Espinal MA, et al. JAMA 2000; 283:2537-45. • A rapid RIF drug resistance may be verly helpful. Traore H, et al. IJTBLD 2000; 4: 481-4 RESULT: • RIF resistance may be a surrogate marker for MDR, in previously treated cases where MDR prevalence is high.
Estimated MDR-TB Burden • South Africa and Kazakhstan • More than 3,000 MDR-TB in each • Henan and Hubai provinces in China • 1,000 cases in each • Estonia, Litvania, Latvia, two oblasts in Russia • Between 99-248 cases in each • Central and West Europe • Less than 10 cases in each.
WHO Estimation StudyPatients in 2003 Zignol M, et al. Union World Congress, 2005, Late Breaker Session Abstracts
WHO Estimation Study: Introduction • There is no result from more than 100 countries • Previous global estimations1: • There are results for 64 countries. • 272.906 MDR-TB cases (95% CI, 184,948-414,295) • 2.6% of new cases (95% CI, 2.2-3.0) • Estimation for only new cases, for previously treated cases it is not present 1. Dye C et al. J Infect Dis 2002; 185:1197-202
WHO Estimation Study: Restrictions • There is estimated number for previously treated cases • Estimations depend on ratio of registered previously treated cases in 2003 and WHO estimation of total case numbers. • Big countries such as China, India, Russian Federation, no country wide data • MDR-TB ratios are extrapolated from regional surveys • Quality of drug resistance data from previously treated cases • Planned surveys for MDR-TB estimation in new cases
WHO Estimation Study - METHODS (1) • 184 countries included. • Two different multipl regression applied for estimation of MDR-TB incidence in these groups: • New TB cases • Previously treated cases • MDR-TB incidence in new cases • Results are present for 90 countries • Estimations done for other 94 countries • MDR-TB incidence in previously treated cases • Results are present for 78 countries. • Estimations done for other 106 countries • Last surveillance (1999-2000) data was used.
WHO Estimation Study - METHODS (2) • Basically WHO new cases estimation was used. • Nine independent factors were used in regression • Regions of the World (9 epidemiologic region) • Fixed dose drug usage • Gross national income • Percentage of TB patients infected with HIV • Percentage of cases previously treated • Percentage of patients treated successfully • Years of RIF usage • Percentage of patients receiving short cours chemotherapy • Estimation of TB incidence rate
WHO Estimation Study – RESULTS for the year 2003 (1) Zignol M, et al. Union World Congress, 2005, Late Breaker Session Abstracts
WHO Estimation Study – RESULTS for the year 2003 (2) • Regions with highest MDR-TB • Eastern Europe (MDR-TB rate is high) • South East Asia (Big number of TB cases) • Western Pasific (Big number of TB cases) • China, India, Russion Federation • 285,725 (95% CI 185,034-439,255) • 67% of the total MDR-TB cases are here Zignol M, et al. Union World Congress, 2005, Late Breaker Session Abstracts
MDR-TB Estimation in the World, 2003 9 epidemiological regions of WHO Global burden: 458.359
MDR-TB Prevalence • MDR-TB prevalence It is estimated 3 times incedence. Blower SM, Chau T. Nature Medicine, 2004; 10:1111-6.
1996 1999 2006