Download
1 / 7
70 likes | 314 Views
Algorithm & Checklist PDSA Trials. Dale Reisner , MD Medical Director of Obstetrics Quality and Safety Swedish Medical Center WSHA Safe Table Safe Deliveries Roadmap November 19, 2013. Presented at Washington State Hospital Association Safe Table 11/19/2013. Induction

E N D
Algorithm & Checklist PDSA Trials Dale Reisner, MD Medical Director of Obstetrics Quality and Safety Swedish Medical Center WSHA Safe Table Safe Deliveries Roadmap November 19, 2013 Presented at Washington State Hospital Association Safe Table 11/19/2013
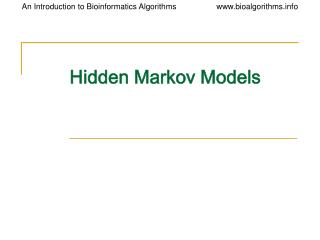
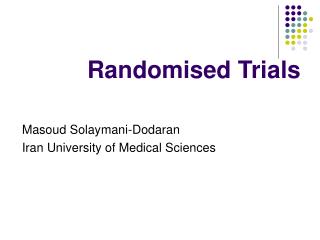
Induction Fetal and Maternal Assessment Appropriate for Induction Draft Medically Indicated Only Favorable Cervix (Bishop Score > 8) Unfavorable Cervix (Bishop Score < 8) Initiate Oxytocin Mechanical or Pharmacological Cervical Ripening DRAFT Cervical Change No Cervical Change No Cervical Change Continue Oxytocin or AROM Repeat with Different Method Cervix < 6 cm, Unable to AROM, or no Cervical Change with 24 Hours Oxytocin Cervix > 6 cm* *may observe for spontaneous labor No Response Oxytocin Trial? If Elective, Consider Home Home or Cesarean See Spontaneous Labor Algorithm Assess Cervical Change • No Change • Adequate contractions • for > 4 hours • Inadequate contractions • for 6 hours Cervical Change Failed Induction Second Stage Arrest Proceed to Cesarean Presented at Washington State Hospital Association Safe Table 11/19/2013
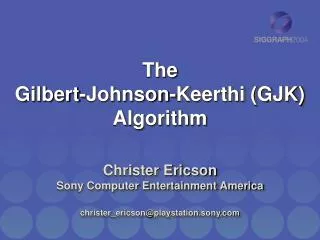
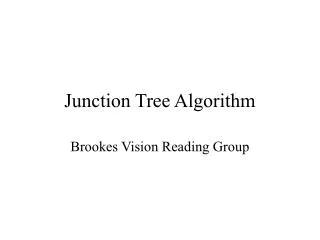
Labor Induction Checklist - DRAFT • Type of Induction: • Medical ___________________________ • Non-medical/Elective • Pre-procedure: • Consent form discussed with patient and signed, and on chart (medical and non-medical) • Non-medical Induction: • Not done prior to 39 weeks gestation. Gestational age: wks_________ days__________ • Between 39 – 40 6/7 weeks gestation, Bishop score is 8 or greater confirmed by 2 examiners (no cervical ripening) • Medical Induction: • Done for accepted medical inductions w/i evidenced-based or National association guidelines (ACOG, SMFM, etc) for definition and most appropriate gestational age for delivery. • Consultation for indication not on above lists • Cervical ripening for unfavorable cervix • Failed Induction (assuming stable mother and fetus) – parameters to use when not entering active labor (> 6 cms): • Either: failure to achieve uterine contractions every 3 minutes with cervical change after 24 hrs of Pitocin and with AROM (if no contraindications), or, uterine contractions every 3 min x 24 hrs without entering active phase if initial Bishop score was less than 8 or if cervical ripening was used. • Inadequate response to a needed, clinically appropriate, second cervical ripening agent • Membranes have ben ruptured with inadequate progress (assuming feasible and no contraindications to AROM) • Pitocin has been given per hospital protocol if inadequate frequency and/or intensity of contractions occur after cervical ripening alone • If ROM, Pitocin given x 12 hrs without regular contractions resulting in cervical change • If Failed Induction: • Options discussed regarding further management: consideration of risks, benefits, and alternatives of all options (i.e. discharge home with plan to return versus Caesarean Section, depending on clinical situation) DRAFT Presented at Washington State Hospital Association Safe Table 11/19/2013
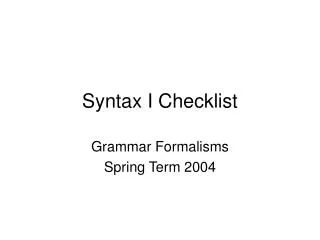
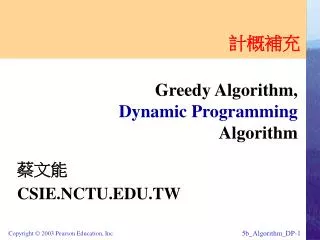
Maternal or Fetal Indication for Admission TRIAGE Induction Algorithm Draft Spontaneous Labor > 37 wks and < 41 wks Stable Mother and Baby Cervix < 4 cm Cervix 4 cm or More DRAFT Inadequate Progress First Stage Walk and Reassess Admit to L&D Home Adequate Progress First Stage First Stage Arrest Operative Vaginal or Cesarean Depending on assessment; Home, AROM and/or Oxytocin, or Cesarean Vaginal Delivery Adequate Progress Second Stage Inadequate Progress Second Stage Adequate Progress Second Stage Inadequate Progress Second Stage Second Stage Arrest Presented at Washington State Hospital Association Safe Table 11/19/2013
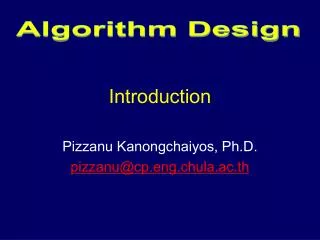
Spontaneous Labor Checklist - DRAFT • First Stage: • Admission delayed for (all conditions met for discharge): • Cervix less than 4 cm • Membranes intact • Reactive NST/FHR category I (if uterine contractions present). Confirmed by 2 practitioners (RN, MD, DO, CNM) • Pain control adequate with appropriate outpatient interventions as needed • Admitted to Labor and delivery (delay admission criteria not met) • Discharged home for: • Cervix 4-5 cm without change x 2-4 hrs • < 80% effacement • Reactive NST/FHR category I (if uterine contractions present) • Contractions less than 3/10 minutes • Further observation for: • Cervix 4-5 cm without change x 2-4 hrs • 90 – 100% effacement • Membranes intact • Reactive NST/FHR category I (if uterine contractions present) • Contractions less than 3/10 minutes • Cesarean delivery for (all criteria present) • Cervix 6 cm or greater • Membranes ruptured (if feasible) • Uterine activity • >200 Montivideountis x 4 hrs, or every 3 minutes palpabley strong contractions x 4 hrs when not feasible to rupture membranes • OR • <200 Montivideo units or <3/10 minute contractions x 6 hrs despite Oxytocin administration per protocol • Second Stage: • Assessment of decent and position of presenting part at least every 1-2 hrs • Operative vaginal delivery or Cesarean delivery for (if presenting part not on perineal floor: +4 or lower) • Time from complete dilation*/** • Nulliparous with epidural - 4 hrs • Nulliparous without epidural - 3 hrs • Multiparous with epidural - 3 hrs • Multiparous without epidural – 2 hrs • OR • Total time from complete dilation 5 hours or greater • > 2 hrs, adequate pattern, no descent • *Passive decent (laboring down) is included in these time periods • **Each may need an additional hour if occiput posterior position and rotation of greater than 45 degrees toward anterior has been previously achieved DRAFT Presented at Washington State Hospital Association Safe Table 11/19/2013
PDSA on 4 Campuses Nov 2013Both sets of Algorithms & Respective Checklists • 29 Algorithms/Checklists evaluated • 27 RNs or LIPs • Common Themes • What to do for <4cms with pain • 4-5 cms but not in labor • Do we suggest the amt of walk & reassess time? • ?SROM: Induction vs Augmentation • Should we note effacement, station? • Are there separate considerations based on parity? • Can a little more guidance be put into algorithms but still keep them easy to follow? Presented at Washington State Hospital Association Safe Table 11/19/2013
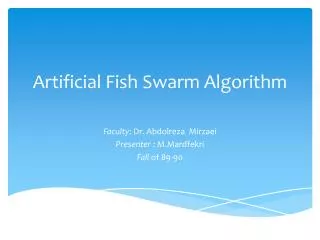
Indication for Induction see Induction Algorithm and Checklist Maternal or Fetal Indication for Admission either in Labor or Needs Induction TRIAGE Spontaneous Labor > 37wks Stable Mother and Baby Assess Exam and Pain New New Cervix < 4 cm Draft Cervix 4 cm or More in Labor DRAFT Inadequate Progress First Stage Walk and Reassess Admit to L&D Home Adequate Progress First Stage First Stage Arrest New Operative Vaginal or Cesarean Depending on assessment; Home vs AROM and/or Oxytocin vs Cesarean Vaginal Delivery Adequate Progress Second Stage • Definitions • Examples: • Adequate progress • reVITALize Inadequate Progress Second Stage Second Stage Arrest Presented at Washington State Hospital Association Safe Table 11/19/2013