Download

1 / 26
280 likes | 591 Views
Influenza Virus. Objectives. Outline the structure of influenza viruses Identify and explain the four diagnostic methods available for detection influenza virus Explain the virulence associated with the influenza virus Discuss the pathophysiology of the virulence factor

E N D
Objectives • Outline the structure of influenza viruses • Identify and explain the four diagnostic methods available for detection influenza virus • Explain the virulence associated with the influenza virus • Discuss the pathophysiology of the virulence factor • Discuss the pharmacology of Oseltamivir • Explain the rational for adding antibacterials to the therapy
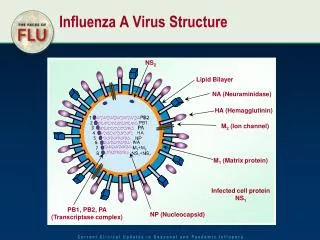
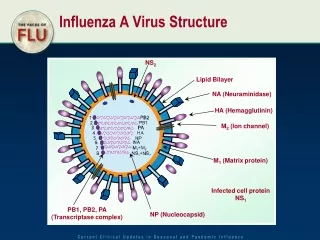
Structure of Influenza Viruses • The physical structure of all Influenza A viruses is similar. • The virions or virus particles are enveloped and can be either spherical or filamentous in form • The influenza virion (as the infectious particle is called) is roughly spherical. It is an enveloped virus – that is, the outer layer is a lipid membrane which is taken from the host cell in which the virus multiplies. • Inserted into the lipid membrane are ‘spikes’, which are proteins – actually glycoproteins, because they consist of protein linked to sugars – known as HA (hemagglutinin) and NA (neuraminidase)
These are the proteins that determine the subtype of influenza virus (A/H1N1, for example). • Beneath the lipid membrane is a viral protein called M1, or matrix protein. This protein, which forms a shell, gives strength and rigidity to the lipid envelope. • Within the interior of the virion are the viral RNAs – 8 of them for influenza A viruses. These are the genetic material of the virus; they code for one or two proteins. • Each RNA segment, as they are called, consists of RNA joined with several proteins shown in the diagram: B1, PB2, PA, NP. These RNA segments are the genes of influenza virus.
The interior of the virion also contains another protein called NEP.
Viral Culture • In this test, the influenza virus is actually grown and identified in the laboratory. • Growing the virus in culture is useful for documenting which strains of influenza are circulating in the community and which antiviral agents are effective in treating these viruses
Direct Fluorescent Antibody Stain (DFA) • This detects influenza A or B virus in samples of nasal secretions. • This method of testing is more specific than RIDT but requires specialized equipment to perform and special training to interpret, so it is usually not performed in a doctor's office. • Samples are typically sent to a laboratory for testing. • If positive, influenza A can be distinguished from influenza B with this method, and results may be available within several hours after the specimen is collected so the appropriate antiviral therapy can be initiated.
Real-time polymerase chain reaction (RT-PCR) • Molecular testing available that detects viral genetic material in nasal secretions and is the most sensitive test for influenza virus. • However, this test is not widely available and results can take from one to several days. • These tests may be ordered to diagnose influenza A infection, especially in those who are seriously ill (hospitalized) and to help track influenza outbreaks.
Rapid influenza diagnostic tests (RIDTs) • These are immunoassays that can identify the presence of influenza A and B viral nucleoprotein antigens in respiratory specimens, and display the result in a qualitative way (positive vs. negative). • The reference standards for laboratory confirmation of influenza virus infection are reverse transcription-polymerase chain reaction (RT-PCR) or viral culture. • RIDTs can yield results in a clinically relevant time frame, i.e., approximately 15 minutes or less. • However, RIDTs have limited sensitivity to detect influenza virus infection and negative test results should be interpreted with caution given the potential for false negative results. • Rapid tests vary in their ability to detect influenza. Some types can only detect influenza A; others can detect both A and B but not distinguish between the two. Still others can detect and distinguish between influenza A and B. However, none of them are able to differentiate between the strains of influenza A, such as H1N1.
Virulence Associated with the Influenza Virus • Definition of virulence:Is the ability of an organism to cause diseases. They usually cause diseases by there expression of virulence factors which are molecules expressed and secreted by pathogens (bacteria, viruses, fungi and protozoa) that enable them to achieve the following: • colonization of a niche in the host (this includes adhesion to cells). • Immunoevasion, evasion of the host's immune response. • Immunosuppressant, inhibition of the host's immune response • entry into and exit out of cells (if the pathogen is an intracellular one). • obtain nutrition from the host.
Associated virulence includes: • Direct viral pneumonia • Secondary bacterial pneumonia • Bronchitis
Viral Pneumonia • Common causes of viral pneumonia are Influenza virus A and B. • The virus will reach the lungs by traveling in droplets through the mouth and nose with inhalation. • There, the virus invades the cells lining the airways and the alveoli. • This invasion leads to cell death either through direct killing by the virus or by self-destruction through apoptosis. • Further damage to the lungs occurs when the immune system responds to the infection. • White blood cells, in particular lymphocytes, are responsible for activating a variety of chemicals (cytokines) which cause leaking of fluid into the alveoli. • The combination of cellular destruction and fluid-filled alveoli interrupts the transportation of oxygen into the bloodstream.
Secondary Bacterial Pneumonia • Secondary bacterial pneumonia is a common cause of death in persons with seasonal influenza. • Secondary bacterial pneumonia occurs after the patient has begun to recover from influenza infection. • The pneumonia was caused when bacteria (such as streptococcus) that normally inhabit the nose and throat invaded the lungs along a pathway created when the virus destroyed the cells that line the bronchial tubes and lungs. • The influenza virus follows the same sequence of events outlined above and makes the body more susceptible to bacterial infection; for this reason, bacterial pneumonia often complicates viral pneumonia.
Acute Bronchitis • Bronchitis describes inflammation of the bronchial tubes. • The inflammation causes swelling of the lining of these breathing tubes, narrowing the tubes and promoting secretion of inflammatory fluid. • Acute bronchitis is manifested by fever, hypertrophy or increase in the size of the mucus secreting tissues, productive cough, sore throat, chills, runny nose. • About 90% of cases of acute bronchitis are caused by viruses, including rhinoviruses, adenoviruses, and influenza. • The influenza virus affects mainly epithelial cells lining the bronchi hence the manifestation of the signs and symptoms specific to this diseases. • The mechanism of action in which the influenza virus causes acute bronchitis is again similar to that which is stated above.
Pathophiology of the Virulence Factor • Influenza viruses are encapsulated, negative-sense, single-stranded RNA viruses of the family Orthomyxoviridae. • The core nucleoproteins are used to distinguish the 3 types of influenza viruses: A, B, and C. • Influenza A viruses cause most human and all avian influenza infections.
The RNA core consists of 8 gene segments surrounded by a coat of 10 (influenza A) or 11 (influenza B) proteins. Immunologically, the most significant surface proteins include hemagglutinin (H) and neuraminidase (N). • Hemagglutinin and neuraminidase are critical for virulence, and they are major targets for the neutralizing antibodies of acquired immunity to influenza. • Hemagglutinin binds to respiratory epithelial cells, allowing cellular infection. • Neuraminidase cleaves the bond that holds newly replicated virions to the cell surface, permitting the spread of the infection
The most common subtypes of human influenza virus identified to date contain only hemagglutinin 1, 2, and 3 and neuraminidases 1 and 2. • These variants result in much of the species specificity due to differences in the receptor usage (specifically sialic acid, which binds to hemagglutinin and which is cleaved by neuraminidase when the virus exits the cell).
Avian viruses tend to prefer sialic acid alpha(2-3) galactose, which, in humans, is found in the terminal bronchi and alveoli. • Conversely, human viruses prefer sialic acid alpha(2-6) galactose, which is found on epithelial cells in the upper respiratory tract.
Pharmacology of Oseltamivir • Oseltamivir (Tamiflu) is indicated for the treatment of uncomplicated acute illness due to influenza infection in patients 1 year and older that has been symptomatic for no more than 2 days. It is also used for the prophylaxis of influenza in adult patients and adolescents 13 years and older.
Oseltamivir is an antiviral drug, a neuraminidase inhibitor used in the treatment and prophylaxis of both influenza A and influenza B. • Oseltamivir is a prodrug (usually administered as phosphate), it is hydrolysed hepatically to the active metabolite, the free oseltamivir carboxylate. • Oseltamivir acts as a transition-state analogue inhibitor of influenza neuraminidase. • The proposed mechanism of action of oseltamivir is inhibition of influenza virus neuraminidase with the possibility of alteration of virus particle aggregation and release. • This result in the inhibition of budding of new virion, therefore halting infection.
It is given orally- capsule/syrup- 75mg bid for 5 days • powder for suspension- 12 mg/mL • Converted in the liver to active compound (oseltamivir carboxylate) • well distributed in the body • t ½ = 6-10 hrs • Eliminated renally • ADR: hepatitis, S-J syndrome • Allergic rxn =anaphylaxis
Rational for Adding Antibacterials to the Therapy • Ventilator associated pneumonia, which results from the invasion of bacteria by intubation. • Intubation compromises the integrity of the oropharynx and trachea which results in the invasion of these microorganisms. • Sepsis (blood poisoning) can occur as a result of bacterial infections. The infectious agents, infects almost any organ location ( including the lungs) or implanted device.
Since the patient already had several cases of clinical sepsis and pneumonia when on mechanical ventilation, then possibly reintubation could result in the reoccurrence of these bacterial infections. • Therefore broad spectrum antibacterial can be given for prophylaxis from these infection and others, as well as, possible treatment of the fever and nonproductive cough (which also could be due to a bacterial infection)
And THE END!!!!!!