Download
1 / 33
330 likes | 516 Views
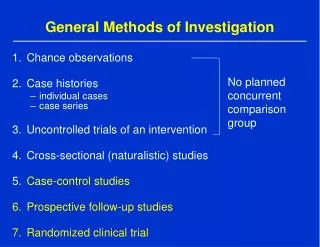
The main methods of investigation of cardiovascular system. Fibrinogen and Atherosclerosis. Promotes atherosclerosis Essential component of platelet aggregation Relates to fibrin deposited and the size of the clot Increases plasma viscosity May also have a proinflammatory role

E N D
Fibrinogen and Atherosclerosis • Promotes atherosclerosis • Essential component of platelet aggregation • Relates to fibrin deposited and the size of the clot • Increases plasma viscosity • May also have a proinflammatory role • Measurement of fibrinogen, incl. Test variability, remains difficult. • No known therapies to selectively lower fibrinogen levels in order to test efficacy in CHD risk reduction via clinical trials.
Fibrinogen and CHD Risk: Epidemiologic Studies • Recent meta-analysis of 18 studies involving 4018 CHD cases showed a relative risk of CHD of 1.8 (95% CI 1.6-2.0) comparing the highest vs lowest tertile of fibrinogen levels (mean .35 vs. .25 g/dL) • ARIC study in 14,477 adults aged 45-64 showed relative risks of 1.8 in men and 1.5 in women, attenuated to 1.5 and 1.2 after risk factor adjustment. • Scottish Heart Health Study of 5095 men and 4860 women showed fibrinogen to be an independent risk factor for new events--RRs 2.2-3.4 for coronary death and all-cause mortality.
AHA / CDC Scientific StatementMarkers of Inflammation and Cardiovascular Disease: Applications to Clinical and Public Health PracticeCirculation January 28, 2003“Measurement of hs-CRP is an independent marker of risk and may be used at the discretion of the physician as part of global coronary risk assessment in adults without known cardiovascular disease. Weight of evidence favors use particularly among those judged at intermediate risk by global risk assessment”.
Fibrinogen and CHD Risk Factors • Fibrinogen levels increase with age and body mass index, and higher cholesterol levels • Smoking can reversibly elevated fibrinogen levels, and cessation of smoking can lower fibrinogen. • Those who exercise, eat vegetarian diets, and consume alcohol have lower levels. Exercise may also lower fibrinogen and plasma viscosity. • Studies also show statin-fibrate combinations (simvastatin-ciprofibrate) and estrogen therapy to lower fibrinogen.
Effects of Weight Loss on CRPConcentrations in Obese Healthy Women • 83 women (mean BMI 33.8, range 28.2-43.8 kg/m2) placed on very low fat, energy-restricted diet (6.0 MJ, 15% fat) for 12 weeks • Baseline CRP positively associated with BMI (r=0.281, p=0.01) • CRP reduced by 26% (p<0.001) • Average weight loss 7.9 kg, associated with change in CRP • Change in CRP correlated with change in TC (r=0.240, p=0.03) but not changes in LDL-C, HDL-C, or glucose • At 12 weeks, CRP concentration highly correlated with TG (r=0.287, p=0.009), but not with other lipids or glucose Heilbronn LK et al. Arterioscler Thromb Vasc Biol 2001;21:968-970.
A Randomized Trial of Rosuvastatin in the Prevention of Cardiovascular Events Among 17,802 Apparently Healthy Men and Women With Elevated Levels of C-Reactive Protein (hsCRP): The JUPITER Trial Paul Ridker*, Eleanor Danielson, Francisco Fonseca*, Jacques Genest*, Antonio Gotto*, John Kastelein*, Wolfgang Koenig*, Peter Libby*, Alberto Lorenzatti*, Jean MacFadyen, Borge Nordestgaard*, James Shepherd*, James Willerson, and Robert Glynn* on behalf of the JUPITER Trial Study Group An Investigator Initiated Trial Funded by AstraZeneca, USA * These authors have received research grant support and/or consultation fees from one or more statin manufacturers, including Astra-Zeneca. Dr Ridker is a co-inventor on patents held by the Brigham and Women’s Hospital that relate to the use of inflammatory biomarkers in cardiovascular disease that have been licensed to Dade-Behring and AstraZeneca.
CRP Improves Net Reclassification Index • From the Physicians Health Study: hs CRP and parental history improved risk prediction 5.3% overall and 14.2% for patients at intermediate risk by traditional risk scores (both P<0.001) (Ridker et al., Circulation 2008) • Framingham Heart Study: hs-CRP improved prediction of cardiovascular disease by 5.6% (P=0.014) and of coronary heart disease by 11.8% (P=0.009) (Wilson et al. Circulation: Cardiovascular Quality and Outcomes 2008).
Homocysteine • Intermediary amino acid formed by the conversion of methionine to cysteine • Moderate hyperhomocysteinemia occurs in 5-7% of the population • Recognized as an independent risk factor for the development of atherosclerotic vascular disease and venous thrombosis • Can result from genetic defects, drugs, vitamin deficiencies, or smoking
Homocysteine • Elevated levels appear to be an independent risk factor, though less important than the classic CV risk factors • Screening recommended in patients with premature CV disease (or unexplained DVT) and absence of other risk factors • Treatment includes supplementation with folate, B6 and B12
Current Biomarkers for ACS • Biomarker assessment of high risk patients may include: • Inflammatory cytokines • Cellular adhesion molecules • Acute-phase reactants • Plaque destabilization and rupture biomarkers • Biomarkers of ischemia • Biomarkers of myocardial stretch (BNP) • Biomarkers of myocardial necrosis (Troponin, CK-MB, Myoglobin) Apple Clinical Chemistry March 2005
History: Troponin • Troponin I first described as a biomarker specific for AMI in 19871; Troponin T in 19892 • Now the biochemical “gold standard” for the diagnosis of acute myocardial infarction via consensus of ESC/ACC 1 Am Heart J 113: 1333-44 2 J Mol Cell Cardiol 21: 1349-53
Troponins • Elevated serum levels are an independent predictor of prognosis, morbidity and mortality • Meta-analysis of 21 studies involving ~20,000 patients with ACS revealed that those with elevated serum troponin had 3x risk of cardiac death or reinfarction at 30 days1 1 Am J Heart (140): 917
BNP • BNP has also shown utility as a prognostic marker in acute coronary syndrome • It is associated with increased risk of death at 10 months as concentration at 40 hours post-infarct increased • Also associated with increased risk for new or recurrent MI
B-Type Natriuretic Peptides and CVD Risk (Circulation 2009; 120: 2177-2187) • Meta-analysis of 40 long-term prospective studies involving 87,474 patients. • Highest vs. lowest tertile, adjusted RR=2.82 (2.40-3.33). • RRs similar for BNP (2.89) or NT-pro BNP (2.82) and in general populations (2.68), increased risk factors (3.35), and stable CVD (2.60). • Modest improvements in risk discrimination (increase in C-statistic of 0.01 to 0.1).
Myeloperoxidase • MPO is an enzyme that aids white blood cells in destroying bacteria and viral particles • MPO catalyzes the conversion of hydrogen peroxide and chloride ions (Cl-) into hypochlorous acid • Hypochlorous acid is 50 times more potent in microbial killing than hydrogen peroxide • MPO is released in response to infection and inflammation • EPIC Norfolk Study showed its predictive value for future cardiovascular disease events in asymptomatic adults. Sugiyama Am J Pathology 2001
A Multimarker Approach Should Focus on Multiple Mechanisms / Pathologies Circulation 108: 250-252
Summary of MPO and ACS • MPO leads to oxidized LDL cholesterol • Oxidized LDL is phagocytosed by macrophages producing foam cells* • MPO leads to the consumption of nitric oxide • Vasoconstriction and endothelial dysfunction • MPO can cause endothelial denuding and superficial platelet aggregation • MPO indicates activated immune cells • Activated immune cells and inflammation lead to unstable plaque* • Inflammatory plaque is inherently less stable • Thin fibrous cap/fissured/denuded Brennan, NEJM 2003 *Hansson, NEJM 2005
The Future of Cardiac Biomarkers • Many experts are advocating the move towards a multimarker strategy for the purposes of diagnosis, prognosis, and treatment design • As the pathophysiology of ACS is heterogeneous, so must be the diagnostic strategies
An Integrated Strategy Multiple Biomarkers Non-redundant pathobiology Intermediate Risk Low Risk
Potential Components of a“Multimarker” Approach Daniels LB. Curr CV Risk Rep 2009.
Malmö, SwedenPopulation-based cohort free of CVD at baseline (n=4483, mean age 58) • 5 biomarkers assessed in backward elimination models • CRP, cystatin C, LP-PLA2, MR-proADM, MR-proANP, NT-proBNP • Results: • 2 markers retained for CVD events • NT-proBNP and CRP • 2 markers retained for CHD events • NT-proBNP and MR-proADM Melander et al. JAMA 2009.