Download
1 / 61
610 likes | 876 Views
VESTIBULAR DISORDERS. Joannalyn B. Juego. ANATOMY: Peripheral Vestibular System. Stabilizing the visual images on the fovea of the retina during head movements to allow clear vision Maintaining postural stability Providing information used for spatial orientation.

E N D
VESTIBULAR DISORDERS Joannalyn B. Juego
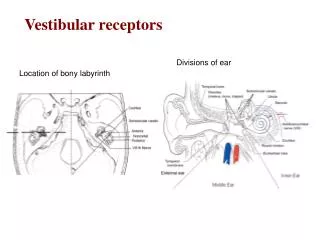
ANATOMY: Peripheral Vestibular System • Stabilizing the visual images on the fovea of the retina during head movements to allow clear vision • Maintaining postural stability • Providing information used for spatial orientation
ANATOMY: Peripheral Vestibular System • Semicircular canals • Otolith organs • Central vestibular system
Vestibular System Dysfunction • Peripheral Pathology • Central Nervous System Pathology
Peripheral Pathology: Mechanical • BPPV • Most common cause of vertigo • A biomechanical disorder • Nystagmus & vertigo without change in head position; nausea with or without vomiting; & dysequilibrium • Latency to onset of the vertigo & nystagmus occurs within 15 seconds once the head is in the provoking position; the duration is less than 60 seconds
Cupulolithiasis • Fragments of the otoconia break away & adhere to the cupula of one of the SCCs • When the head is moved into certain positions, the weighted cupula is deflected by the pull of gravity • The abnormal signal results in vertigo & nystagmus, which persists as long as the patient is in the provoking position
Canalithiasis • Otoconia are freely floating in one of the SCCs • When a patient changes head position, the pull of gravity causes the freely floating otoconia to move inside the SCC resulting in endolymph movement & deflection of the cupula
Peripheral Pathology: Decreased Receptor Input • UVH • Viral insults, trauma, & vascular events • Vertigo, spontaneous nystagmus, oscillopsia during head movements, postural instability, & dysequilibrium • Resolves within 3-7 days assuming the patient is exposed to common daylight conditions
Peripheral Pathology: Decreased Receptor Input • BVH • Ototoxicity • Meningitis, autoimmune DO, head trauma, tumors on the 8th CN, transient ischemic episodes of vessels supplying the vestibular system, & sequential unilateral vestibular neuronitis • Dysequilibrium, oscillopsia, & gait ataxia
Central Nervous System Pathology • Cerebrovascular insults involving the AICA, PICA, & vertebral artery • Vertebrobasilar insufficiency (VBI) • TBI due to labyrinthine or skull fractures • Demyelinating diseases such as MS affecting CN VIII
PHYSICAL THERAPY EXAMINATION • History & Systems Review • Identification of symptoms • Duration & circumstances of symptoms
Identification of Symptoms • Dizziness • Vaguely defined as the sensation of whirling or feeling a tendency to fall • Patients should be directed away from using the word & to use more precise terms • Vertigo, lightheadedness, dysequilibrium, oscillopsia
Vertigo • Illusion of movement • Episodic • Indicates pathology at one or more locations along the vestibular pathways • Acute stage of UVH • Displaced otoconia (BPPV) • Acute unilateral brainstem lesion
Lightheadedness • Feeling that fainting is about to occur • Causes • Orthostatic hypotension • Hypoglycemia • Anxiety • Panic disorder
Dysequilibrium • Sensation of being off balance • Causes • BVH • Chronic unilateral vestibular hypofunction • Lower extremity somatosensation loss • Upper brainstem/vestibular cortex lesion • Cerebellar & motor pathway lesions
Oscillopsia • Subjective experience of motion of objects in the visual environment that are known to be stationary • Occur with head movements in patients with vestibular hypofunction since the vestibular system is not generating an adequate compensatory eye velocity during the head motion
Duration & Circumstances of Symptoms • How recent the attacks happened • Whether the symptom is constant or episodic • Episodic: average duration of the episodes • Seconds to minutes – BPPV • Minutes to hours – Meniere’s disease • Days – vestibular neuronitis or migraine-associated dizziness
Duration & Circumstances of Symptoms • Whether the patient experiences symptoms with particular movements, positions, or at rest • Is the patient sensitive to motion as the passenger in a moving car? • Does the patient experience a vigorous vertigo when the head is moved into certain positions?
Tests & Measures • Visual Analogue Scale • Dizziness Handicap Inventory • Functional Disability Scale • Vestibular Rehabilitation Benefit Questionnaire • Motion Sensitivity Quotient • Examination of Eye Movements
Observation for Nystagmus • Nystagmus is the primary indicator used in identifying most peripheral & central vestibular lesions • The direction of the nystagmus is named by the direction of the fast component • Left beating nsytagmus: eyes move slowly to the right & the resetting eye movement is to the left
Head Impulse Test (Examination of the VOR at High Acceleration) • Widely accepted clinical tool used to examine semicircular canal function • Patient first fixates on a near target • When testing the horizontal SCC, the head is flexed to 30 deg
Head Impulse Test (Examination of the VOR at High Acceleration) • Patient is asked to keep their eyes focused on a target while his head is manually rotated in an unpredictable direction using a • Small amplitude (5 – 15 deg), • Moderate velocity (~200 deg/sec), and • High-acceleration (3,000 – 4,000/sec) angular impulse
Head Impulse Test (Examination of the VOR at High Acceleration) • Normal • Eyes will move in the direction opposite to the head movement & gaze will remain on the target • With a loss of vestibular function • The VOR will not move the eyes as quickly as the head rotation & the eyes will move off the target • The patient will then make a corrective saccade to reposition the eyes on the target • Corrective saccade: rapid eye movement used to reposition the eyes to the target of interest
Head Impulse Test (Examination of the VOR at High Acceleration) • Unilateral peripheral lesion or pathology of the central vestibular neurons • Patient will not be able to maintain gaze when the head is rotated quickly toward the side of the lesion • Bilateral loss of vestibular function • Patient will make corrective saccades after a head impulse to either side
Head-Shaking Induced Nystagmus Test (HSN) • Useful aid in the diagnosis of a unilateral peripheral vestibular defect • Patient is instructed to close his eyes • Clinician flexes the head 30 deg before oscillating horizontally for 20 cycles at a frequency of 2 repetitions per second • On stopping the oscillation, the patient opens the eyes & the clinician checks for nystagmus
Head-Shaking Induced Nystagmus Test (HSN) • Normal • Nystagmus will not be present • Presence of asymmetry between the peripheral vestibular inputs to central vestibular nuclei • May result in HSN • UVH • Horizontal HSN • Quick phases of the nystagmus directed toward the healthy ear & the slow phases directed toward the lesioned ear
Positional Testing • Commonly used to identify whether otoconia have been displaced into the SCC, causing a condition referred to as Benign Paroxysmal Positional Vertigo (BPPV) • Dix-Hallpike Test • Patient is moved from a long-sitting position with the head rotated 45 deg to one side, to a supine position with the head extended to 30 deg beyond horizontal, head still rotated to 45 deg • Observe the eyes for nystagmus
Positional Testing • Dix-Hallpike Test Side-lying • Patient sits on the edge of the examination table • Clinician turns the head horizontally 45 deg • Patient is quickly brought down to the side opposite the head rotation • Examiner checks for nystagmus & vertigo, & then slowly brings the patient to the starting position • The other side is then tested
Positional Testing • Roll test • If horizontal SCC BPPV is suspected • Patient is positioned supine with the head flexed 20 deg • Rapid rotations to the sides are done separately & the clinician observes for nystagmus & vertigo
Dynamic Visual Acuity (DVA) Test • Measurement of visual acuity during horizontal motion of the head • Static visual acuity is first determined • Patient is asked to “Read the lowest line you can see” on a wall-mounted acuity chart • Lighthouse ETDRS (Early Treatment Diabetic Retinopathy Study) wall charts are recommended • Patient then attempts to read the chart while the clinician horizontally oscillates the patient’s head at a frequency of 2Hz
Dynamic Visual Acuity (DVA) Test • Normal • Head movement results in little or no change of visual acuity compared with the head still (less than 1 line difference) • Loss of vestibular function • Eyes will not be stable in space during head movements • Decrement in DVA compared with visual acuity when the head is still • A 3-line or more decrement in visual acuity during head movement is suggestive of vestibular hypofunction
Vestibular Function Tests: Semicircular Canal Tests • Electronystamography (ENG) & Videonystamography (VNG) • Oculomotor & inner ear function • Rotational chair test • Rotating subjects in the dark • Standard test for bilateral vestibular dysfunction
Vestibular Function Tests: Otolith Tests • Vestibular-evoked myogenic potential (VEMP) • Cervical VEMP • Ocular VEMP
Benign Paroxysmal Positional Vertigo • The otoconia will be returned into the vestibule • The patient will demonstrate reduced vertigo associated with head motion • The patient will demonstrate improved balance • The patient will demonstrate independence in ADLs
Benign Paroxysmal Positional Vertigo • Canalith repositioning maneuver (CRM) • BPPV due to canalithiasis, posterior SCC canalithiasisis the most common • Liberatory (Semont) maneuver • BPPV due to cupulolithiasis, posterior SCC cupulolithiasis is the most common • Brandt-Daroff exercises • Persistent/residual or mild vertigo (even after CRM); for the patient who may not tolerate CRM
Unilateral Vestibular Hypofunction • The patient will demonstrate improved stability of gaze during head movement • The patient will demonstrate diminished sensitivity to motion • The patient will demonstrate improved static & dynamic postural stability • The patient will be independent in proper performance of a HEP that includes walking
Unilateral Vestibular Hypofunction • Gaze Stability Exercises • Improve the VOR & other systems that are used to assist gaze stability with head motion • Designed to expose patients to retinal slip
Retinal Slip • Occurs when the image of an object moves off the fovea of the retina, resulting in visual blurring • Necessary as this is the signal used to drive vestibular adaptation within the brain • Because the brain can tolerate small amounts of retinal slip yet see a target clearly, the patient must try to keep the target in focus • Otherwise, head motion that is too rapid will result in excessive retinal slip
Primary Paradigms of Vestibular Adaptation • x1 exercises • Patient is asked to move the head horizontally as quickly as possible while maintaining focus on a stable target • Patient must learn how to slow the head movement if the target becomes blurred • Starting target distance should be an arm’s length away
Primary Paradigms of Vestibular Adaptation • x2 exercises • Requires the patient to move the head & the target in opposite directions