Download

1 / 26
280 likes | 469 Views
Normal Retina. Fovea. Macula. Photoreceptors. RPE. Choroid. A range of visual defects with macular pathology. Neovascular AMD. Neovascular AMD. Distortion. Blur. Scotoma. Normal. DME. DME. DME with proliferative DR. Blur + scotomas. Blur. RISK FACTORS. Age Smoking

E N D
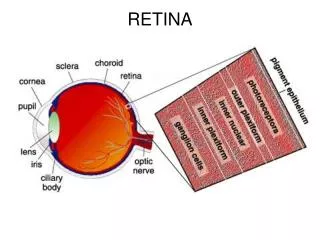
Normal Retina Fovea Macula Photoreceptors RPE Choroid
A range of visual defects with macular pathology Neovascular AMD Neovascular AMD Distortion Blur Scotoma Normal DME DME DME with proliferative DR Blur + scotomas Blur
RISK FACTORS Age Smoking Positive family history Hypertension Females Raised cholesterol Light iris color
DIET Vitamins – C 500 mg, E 400 IU Micronutrients – Zinc 80mg with 2mg cupric oxide Beta carotene 15mg – Avoid in smokers Fish Nuts
Lifestyle modification Avoid smoking Reduce obesity Use sunglass & Hats Avoid alcohol
VEGF Inhibition in AMD FDA approved Pegaptanib Aptamer Specific for VEGF-A isoform 1651 Ranibizumab Recombinant, humanized antibody fragment Blocks all VEGF-A isoforms Off label Bevacizumab Recombinant humanized monoclonal antibody Blocks all VEGF-A isoforms 1Gragoudas ES, et al. N Engl J Med. 2004;351:2805.
VEGF-A Is a Key Mediator of Angiogenesis Environmental factors1 (hypoxia,2 pH) Growth factors, hormones1 (EGF, bFGF, PDGF, IGF-1, IL-1, IL-6, estrogen) VEGF-A binding and activation of VEGF receptor3 Endothelial cell activation3 VASCULARLEAKAGE3 Endothelial cell activation, proliferation, migration4 ANGIOGENESIS3 VEGF-A = vascular endothelial growth factor A; EGF = epidermal growth factor; bFGF = basic fibroblast growth factor; PDGF = platelet-derived growth factor; lGF = insulin-like growth factor; IL= interleukin. 1. Dvorak HF. J Clin Oncol. 2002;20:4368. 2. Aiello LP, et al. Arch Ophthalmol. 1995;113:1538. 3. Ferrara N, et al. Nat Med. 2003;9:669. 4. Griffioen AW and Molema G. PharmacolRev. 2000;52:237.
VEGF Inhibition in AMD FDA approved Pegaptanib Aptamer Specific for VEGF-A isoform 1651 Ranibizumab Recombinant, humanized antibody fragment Blocks all VEGF-A isoforms Off label Bevacizumab Recombinant humanized monoclonal antibody Blocks all VEGF-A isoforms 1Gragoudas ES, et al. N Engl J Med. 2004;351:2805.
Different gold standard diagnostics with common ancillary tests • Early detection of neovascular AMD is possible with an Amsler grid1 • FA is essential to confirm diagnosis of neovascular AMD, and to identify the location and composition of the CNV1 • Ancillary tests:2 • ICGA – delineation of choroidal vessel morphology • OCT – measurement of retinal thickness • DME is diagnosed stereoscopically as retinal thickening in the macula using fundus contact lens biomicroscopy3 • Ancillary tests:3 • FA – identification and evaluation of fluid leakage from lesions • OCT – measurement of retinal thickness Neovascular AMD DME 1. Sickenberg M. Ophthalmologica 2001;215:247–253 2. The Royal College of Ophthalmologists. AMD: guidelines for management. 2009. http://www.rcophth.ac.uk/docs/publications/AMD_GUIDELINES_FINAL_VERSION_Feb_09.pdf [accessed Sep 2009] 3. Bhagat N et al. Surv Ophthalmol 2009;54:1–32
Standard of care: improvement with neovascular AMD vs stabilization with DME • Ocular treatment – Anti VEGFs IVI1 • Maintenance of vision can be expected in 90–95% of patients • Improvement of vision by ≥3 lines can be expected in 30–40% of patients • Ocular treatment – laser photocoagulation2–4 • Rarely provides visual improvement • In the 1985 ETDRS, VA improved in 16%, was unchanged in 77% and worsened in 7% of patients • Systemic treatment4 • Glucose control • Blood-pressure control • Blood-lipid control • Multifactorial metabolic interventions Neovascular AMD DME 1. Schmidt-Erfurth UM et al. Acta Ophthalmol Scand 2007;85:486–494 2. Bhagat N et al. Surv Ophthalmol 2009;54:1–32 3. Early Treatment Diabetic Retinopathy Study research group. Arch Ophthalmol 1985;103:1796–1806 4. Furlani BA et al. Expert Opin Emerg Drugs 2007;12:591–603
Diabetes mellitus (DM) is a prevalent disease. Most common complications are microvascular changes1 Diabetic retinopathy (DR) is a common microvascular complication of diabetes2 Diabetic macula edema (DME) is a common cause of blindness in people of working age2,3and can develop in both Type 1 and 2 DM4 About 8% of diabetic patients develop DME with visual impairment5 Diabetes and vision loss 1King et al. Diabetes Care 1998; 21: 1414-1431; 2Royal College of Ophthalmology. Diabetic Retinopathy Guidelines 2005. http://www.rcophth.ac.uk/docs/publications/publishedguidelines/DiabeticRetinopathyGuidelines2005.pdf. Accessed February 2009; 3Watkins. BMJ 2003; 326: 924-926; 4Klein et al. Ophthalmology 1998; 105: 1801-1815; 5Calculated from: Ling et al. Eye 2002; 16: 140-145; Broadbent et al. Eye 1999; 13: 160-165; Knudsen et al. Br J Ophthalmol 2006; 90: 1404-1409; Hove et al. Acta Ophthalmol Scand 2004; 82: 443-448; Romero-Aroca et al. Arch Soc Esp Oftalmol 2007; 82: 209-218; Zietz et al. Dtsch Med Wochenschr 2000; 125: 783-788; Kristinsson. Acta Ophthalmol Scand Suppl 1997; 223: 1-76
DME: the main cause of central vision loss in DR DME was shown to affect approximately 10% of the diabetic population Klein et al. Ophthalmology 1995; 102: 7-16
VEGF165 in DR Retinal VEGF165 levels are elevated in experimental diabetes Increased VEGF165 levels are found in the vitreous of eyes with proliferative DR Patients with DR have higher VEGF165 levels in the aqueous Qaum et al. IOVS 2001; 42: 2408-2413; Aiello et al. N Engl J Med 1994; 331: 1480-1487
Factors affecting DME Incidence of DME increases with elevated levels of HbA1C severity of DR duration of DM elevated diastolic blood pressure gender (more frequent in females) serum lipid levels Klein et al. Ophthalmology 1998; 105: 1801-1815
DME: current treatment Systemic treatment glucose control blood-pressure control blood-lipid control multifactorial metabolic interventions Ocular treatment laser photocoagulation (standard treatment for DR / DME) vitrectomy pharmacologic therapy AAO Guidelines. Diabetic Retinopathy. http://www.aao.org/ppp. Accessed February 2009 Royal College of Ophthalmology. Diabetic Retinopathy Guidelines 2005. http://www.rcophth.ac.uk/docs/publications/publishedguidelines/DiabeticRetinopathyGuidelines2005.pdf. Accessed February 2009
Reduction in vessel hyperpermeabilityand leakage in macular edema DME: aims of therapy Treatment of neovascularizatio in PDR
Laser photocoagulation for DME National Eye Institute, National Institutes of Health. Diabetic Retinopathy. http://www.nei.nih.gov/health/diabetic/retinopathy.asp#4a Accessed February 2009 AAO Guidelines. Diabetic Retinopathy. http://www.aao.org/ppp. Accessed February 2009 Royal College of Ophthalmology. Diabetic Retinopathy Guidelines 2005. http://www.rcophth.ac.uk/docs/publications/publishedguidelines/DiabeticRetinopathyGuidelines2005.pdf. Accessed February 2009 • Standard treatment – helps to slow fluid leakage and reduce the amount of fluid in the retina (macula edema) • Aim of treatment is to stabilize / prevent further vision loss • Limitations of treatment include • does not eliminate possibility of further vision loss • improvement in visual acuity is uncommon • complications including permanent damage to the retinal pigment epithelium and secondary choroidal neovascularization
DR and DME: the unmet treatment needs Despite the use of standard interventions for DR, vision loss as a result of the disease still occurs in many patients1 Good metabolic and blood-pressure control are often difficult to achieve in clinical practice, and sight-threatening DR still develops2 Laser treatment is destructive and cannot restore vision loss that has already occurred; it therefore cannot be regarded as an ideal treatment, and there is a need for better-tolerated and less-destructive therapies3 1Comer & Ciulla. Curr Opin Ophthalmol 2004; 15: 508-518 2The DIRECT Programme Study Group. J Renin Angiotensin Aldosterone Syst 2002; 3: 255-261 3Fong. Surv Ophthalmol 2002; 47: S238-S245
Intravitreal Ranibizumab Summary Intravitreal ranibizumab with prompt or deferred (≥24 weeks) focal/grid laser had superior VA and OCT outcomes compared with focal/grid laser treatment alone. ~50% of eyes had substantial improvement (≥10 letters) while ~30% gained ≥15 letters Substantial visual acuity loss (≥10 letters) was uncommon Results were similar whether focal/grid laser was given starting with the first injection or it was deferred >24 weeks