Download
1 / 18
190 likes | 638 Views
Management of Osteoarthritis of the Knee. Anoop Agrawal, M.D. Baylor College of Medicine. Background. Knee Osteoarthritis is a slowly developing chronic disease of multifactorial origin. Risk factors include: obesity acute joint injury occupational factors (bending, lifting)

E N D
Management of Osteoarthritis of the Knee • Anoop Agrawal, M.D. • Baylor College of Medicine
Background • Knee Osteoarthritis is a slowly developing chronic disease of multifactorial origin. • Risk factors include: • obesity • acute joint injury • occupational factors (bending, lifting) • genetic - although actual genes and mechanism of association is uncertain
Pathogenesis Loss of articular cartilage Increased focal stress Further loss of cartilage Bony remodeling Joint Malalignment Joint Failure
Diagnosis • Classic clinical criteria: developed in 1986 by an expert panel • It requires the presence of knee pain plus at least 3 of the following 6: • age >50 years • morning stiffness <30 minutes • crepitus on active motion of the knee • bony tenderness • bony enlargement • no palpable warmth
Diagnosis • Classic criteria has sensitivity of 95%, specificity of 69%. • Other classification trees have been developed - some incorporate lab studies and x-ray findings along with clinical features.
Keys to Diagnosis • Pain related to activity is the hallmark. • History of pain with activities involving knee bending indicates disease in the patellofemoral joint • History of knee giving way may indicate an associated meniscal or ACL tear. • Both of these tears are common in advanced OA • Pain at night is indicative of severe OA vs. pain from other causes (tumors, infection, inflammation)
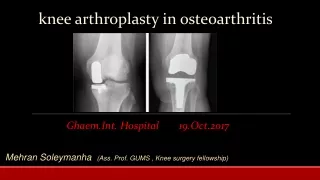
Radiography • True or False. Radiographic findings correlate poorly with the severity of pain. • True, knee films may be normal in patients with osteoarthritis Indications for x-rays in the workup of knee pain: Pain is nocturnal Pain is not activity-related Pain persists after effective therapy of OA
Exam findings • On examination of the leg, is the pain being referred from the hip? • Legs should be examined for malalignment, i.e varus or valgus deformity. • Observe and record the patient’s gait - is there an antalgic gait? Does the patient use a cane? • Is there pain to palpation over the joint lines? • Perform McMurray and Lachman
Laboratory Studies • No lab studies are indicated unless symptoms and signs are suggestive of other pathology. • Synovial fluid examination and serologic markers for inflammation aid in ruling out inflammatory conditions. • Synovial fluid with white cell count below 1000 is consistent with OA.
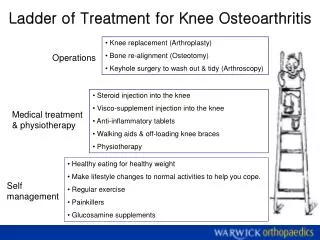
Treatment • Pharmaceutical • Oral analgesics (acetaminophen, NSAIDS) • Injections of Hyaluronic Acid • Glucosamine and Chondroitin Sulfate • Intraarticular corticosteroid injections • Nonpharmaceutical • Exercise, correcting malalignment, unloading, acupuncture, yoga
Oral Analgesics • Which drug is more efficacious in relieving osteoarthritic pain - NSAIDS, COX-2 inhibitors, or acetaminophen? • NSAIDS and COX-2 inhibitors - a 2006 Cochrane analysis review of 15 randomized control trials involving 5,986 patients found these agents superior to acetaminophen • However, because of NSAIDS have greater toxicity (CV, GI), the American College of Rheumatology still considers acetaminophen as first line of therapy.
Oral Analgesics • Acetaminophen also appears to be less effective in patients who have already received therapy with NSAIDs. • PPIs or other GI-protective meds are increasingly being recommended for use with NSAIDs. There is no method to counter the increased cardiovascular risk other than to limit their use.
Other oral agents • Tramadol is a synthetic opioid agonist that binds weakly to mu receptors. • Studies in OA patients have shown tramadol to be comparable to ibuprofen and can be used as an adjunctive in patients who are inadequately controlled with NSAIDS alone. • Opioids are the final oral agent of choice if the patient is not responding to the above therapies
Other pharmaceutical agents • Injection of Hyaluronic Acid - is FDA approved for treatment of OA, however, data from large trials suggest very limited efficacy. • Glucosamine and Chondroitin Sulfate - MOA unclear; good safety profile; no clear benefit • Intraarticular corticosteroid injection - is effective in providing pain relief, duration is variable (1 week to a few months). There is no data regarding optimal number or frequency. • Topical capsaicin - modestly better than placebo
Nonpharmacuetical Therapy • Exercise: specifically, muscle strengthening of quadriceps • helps to improve alignment, stability of the joint and reduces pain. • must be resistance training (isotonic) • Reduce joint-loading forces via use of canes or walkers • Correct malalignment with shoe inserts, knee braces, or neoprene sleeves
Summary • OA of the knee starts with the loss of articular cartilage and results in joint failure • Diagnosis of OA is based on clinical criteria. • Radiography and laboratory testing do not assist in diagnosing OA, but rather in ruling out other disease processes. • Therapy with acetaminophen remains first line, though NSAIDS have somewhat better efficacy. • Instituting nonpharmacologic tx such as resistance training and correcting malalignment are as impotant as pain control in preventing progression.
References • Felson, DT. Osteoarthritis of the Knee. New England Journal of Medicine 2006; 354:841-8. • Katz, WA. Management of Moderate Chronic Pain in Osteoarthritis. Medscape, April 27, 2006. • Kalunian, KC. Brion PH. Wollaston, SJ. Diagnosis and Classification of Osteoarthritis. UpToDate® Online 15.1; 2007. • Tauheed, T. Maxwell, L. Judd, M. et al. Acetaminophen for Osteoarthritis. Cochrane Database Systems Review 2006;(1):CD004257