Download
1 / 21
220 likes | 358 Views
Initial Response Team Sunderland and South of Tyne. Improving Access to Urgent Mental Health Services Dr Paul Brown- NTW Lead Consultant for Access, IRT/ CRHT David Hetherington- Senior Clinician- Sunderland IRT/ CRHT Rachel Winter- Sunderland IRT/ CRHT Clinical Lead. Context

E N D
Initial Response TeamSunderland and South of Tyne Improving Access to Urgent Mental Health Services Dr Paul Brown- NTW Lead Consultant for Access, IRT/ CRHT David Hetherington- Senior Clinician- Sunderland IRT/ CRHT Rachel Winter- Sunderland IRT/ CRHT Clinical Lead
Context Model Development Engagement and Commissioning IRT Evaluation Case Examples and Service User Feedback Overview
Access? • Access is the term used by NTW to describe the Initial Response to Urgent and Routine requests for help. • Urgent Requests – Phase 1- (2012) • Routine Requests – Phase 2- (2014) • Integration with other routes of entry such as… • IAPT • Specialist Services • Social Care
Phase 1: The case for change • Sunderland was chosen as the location for the development of a new access model following discussions with service users, carers, GPs and commissioners. • Clear issues with contacting the Crisis Team by phone as Triage saturated++ • Overnight and at peak demand times callers could wait hours for a return call from a clinician • No ready point of access for Older People or People with a significant Learning Disability seeking Urgent Advice/ Intervention • Fewer than 35% of referrals needed a Crisis Team Response • Most of the “inappropriate” calls required some form of advice/ signposting but at low risk/ acuity
Large scale events- Local Authority, GP’s, Commissioners, Service Users Focussed Group Events- Service Users, GP’s, Staff Engagement
Sunderland PCT facilitated and supported Initial Engagement process Recognised need for change Supported 1st year (Pilot) through imaginative use of CQUIN On basis of initial evaluation have commissioned ongoing service Ongoing development of whole-system Engagement- Commissioners
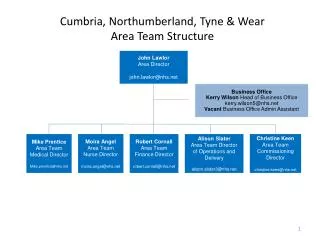
Initial Response Team South of Tyne and Wear Gateshead 11 Home Based Treatment Assessment Gatekeeping Rapid Response Nurses Information Collection & Routing Triage & Action South Tyneside REQUEST FOR HELP GH UCT SL UCT ST UCT 11 Home Based Treatment Assessment Gatekeeping Rapid Response Nurses OPS OPS OPS LD LD LD Triage & Action Sunderland ICTS ICTS ICTS Home Based Treatment Assessment Gatekeeping 11 Rapid Response Nurses ROUTING Triage & Action
Phase 2 Model IRT 11 Rapid Response Nurses Triage Team Home Based Treatment Assessment Gatekeeping Urgent Triage & Action UCT Single Point of Referral OPS LD Clinical Diary Non-complex ICTS Routine Clinical Diary Complex Huddle
Phase 1: The Model • IRT to offer 24/7 Universal telephone access for requests for urgent help. • No restrictions on who could refer • Triage and Routing over the phone- (Mental Health and other local Services) • Face to Face Triage (Rapid Response) if clear plan cannot be determined over the phone • Seven Band 6 Nurses for Telephone and Rapid Response • Five Band 3 Nurses for call handling and Rapid Response • Use of digital dictation and 3G laptops for clinical documentation • Flexible interchangeable roles and rotation between Crisis Team and IRT roles dependant on demand.
Phase 1: Benefits of IRT • Quick and efficient responses to requests for help • Effective routing to the correct services in and out of NTW • Flexible and collaborative working with newly configured UCT which will focus on the work for which it is commissioned • Reduction of clinician administration burden, and freeing time to care (mainly through adoption of digital dictation) • Improving personal and clinical outcomes for people in crisis with mental ill health by reducing harm and premature mortality, improving patient safety and patient experience
Evaluation-IRT in numbers • Typical weekly activity • 1500+ Incoming telephone calls • 1000 Total Contacts • 400 Home-based Treatment contacts • 50 Crisis Assessments • 100 Rapid Responses • …and growing • 90% calls answered within 15 seconds • >98% within 3 minutes (Average=9 Seconds) • >80% rapid responses achieved in under one hour
IRT Referrals (Q3 2013) • Other includes: • Self Harm Team • Acute Care Trust • NTW Inpatient Ward • Ambulance • Consultant Psychiatrist • Residential Care Facility • Drug and Alcohol Services • IAPT • Member of Public • EDT • Probation
Service Feedback Service User and Carer GP I felt listened to and was delighted The service is responsive and friendly I cannot imagine where I would be today if you had not been there for me. You listened and told me what to do Fantastic – a huge improvement!! You should have done it before Keep this very valuable service going I couldn’t have got this far without your help Staff You are all very dedicated, patient, compassionate people More manageable A lot happier You do an amazing job! Skills are valued Spend more time Wonderful support!
“Its because of IRT that I haven’t self harmed in four months. Before, I would self harm two or three times a week and would end up in A&E, but knowing that they are there and knowing that I’m going to get the same positive response every time means that I have been able to listen to their advice and develop coping strategies. I’m much more hopeful about my future” Service User Narrative Feedback
First contact from brother, family concerned ++ “odd” ideas, becoming reclusive Triage completed via Rapid Response (Face to Face) within one hour (after contact with John. Engaged in period of home-treatment- referred to EIP Case Example 1- John- 31
Local Community Police Referral Jenny had been contacting them regularly Concern re mental health and self-neglect Rapid-Response to join police at property Crisis Assessment identified depression, alcohol dependence and social issues Home Treatment Joint work with social care Case Example 2- Jenny 60
IRT developed in a context of shared goals with commissioner and wider partners IRT shown to vastly improve access & responsiveness with widely positive feedback Next steps planned will look at incorporating all referrals and wider system Summary