Download
1 / 27
270 likes | 415 Views
Care Transitions. Ken Wilson N4A July 17, 2011. Cincinnati AAA Experience. Strategic plan: develop program to divert nursing home placement at the time of hospitalization. More than 60% of long term NF placements begin as a post-acute stay. Cincinnati AAA Experience.

E N D
Care Transitions Ken Wilson N4A July 17, 2011
Cincinnati AAA Experience • Strategic plan: develop program to divert nursing home placement at the time of hospitalization. • More than 60% of long term NF placements begin as a post-acute stay.
Cincinnati AAA Experience Problem #1: No source of funding Problem #2: Education of discharge planners doesn’t change behavior Our goal: make hospital discharges to home as easy and seamless as a discharge to a SNF
Cincinnati AAA Experience Solution: Prioritized existing staffing resources to invest in a new department “nursing home diversion and transition”. • Organization restructuring that eliminated positions and departments and created new positions and departments.
Communicating our value Presentations to hospitals and health plans on our value, and the benefits of working with the AAA. Community Leader presentations
Shared Goals, Mutual Benefit Poorly executed care transitions lead to poor clinical outcomes, dissatisfaction among patients, and inappropriate use of hospital, emergency, and post acute services. 1 in 5 are readmitted in 30 days 1 in 3 within 90 days $15 billion cost
Our Motto… the perfect fit The right care, at the right time, in the right setting, at the right cost. “I love being able to stay in my own home. It means something to my heart.” Ruth
Development of our model • Adopted the Coleman Care Transition Model • Integrated Care Transitions with value added services available through our AAA: • Access to community based services • Unbiased information • Care Management
Two Goals • Reduce hospital readmissions • Reduce long term nursing facility placements
Cincinnati Area Hospital • Implementation of the model at the hospital with highest re-admission rate in the state.
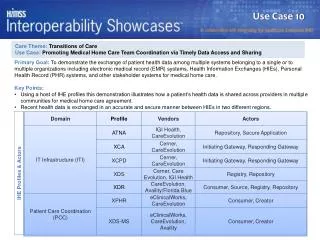
Partnerships Health Information Exchange (HIE) • Electronic Information exchange • Hospitalization alerts/client identification • Shared medical record?
Additional Partnerships Partnerships with two Universities for grant writing, and evaluation. Hospital Council Mental Health Board Executive Service Corps Health Improvement Collaborative Health Care Access Agency Four Hospital Systems
COA Care Transition Model • Coleman CTI evidence-based model • Integration with: • Local Hospitals • Primary Care Physician • Health Information Exchange • COA funded In-home services • Care Coordination • Caregiver Support
Care Transition Clients • Age 60+ • PASSPORT or Hamilton County ESP eligible (chronic care needs) • Admission to a participating hospital: • UC Health • Christ Hospital
Summary of Results • High participation rate (65%) • 28% of clients were admitted with a diagnosis considered to be high risk for readmission by CMS (AMI, CHF, Pneumonia) • 30-day readmission rate of 7.5% for individuals in the COA Care Transitions Intervention (compared to 20% for Medicare fee-for service) • 0% readmission rate for individuals admitted with a high risk diagnosis
Care Transition Participation65% Participation Rate n=106 n=37 Source: Council on Aging of Southwestern Ohio, 6/7/11 n= 106
Care Transition ParticipationEligible vs. Not Eligible • Of those clients eligible for CTI, 86% chose to participate* • To date, 66% have completed CTI. • Of those clients who were not eligible for CTI, • 4.7% would have been a good fit for Naylor, • 3.7% would have been a good fit for a community mental health program, • 9.4% were not identified as a good fit for any specific program/model (as the individual was preparing for a long-term NF stay or were entering Hospice), and • 6.6% fit into the ‘other’ category as they were no eligible because they were no longer a PSP client or were heading to another HCBS program. * Eligible clients include individuals who were admitted to CTI (n=69) and those who were eligible but declined (n=11).
Care Transition Clients Reason for Admission Admission Diagnosis *28% of the total were admitted with a diagnosis considered to be high risk for readmission by CMS. Source: Council on Aging of Southwestern Ohio, 6/7/11 n= 69 COPD: Chronic Obstructive Pulmonary Disease, AMI: Acute Myocardial Infarction, CHF: Congestive Heart Failure.
Secondary Diagnoses • On average, clients had 3.5 secondary diagnoses • The most common secondary diagnoses include: • Hypertension (64.1%) • Diabetes (59.0%) • Congestive Heart Failure (CHF) (30.8%) • Chronic Obstructive Pulmonary Disease (COPD) (25.6%) • Stroke (CVA) (17.9%) • Coronary Artery Disease (CAD) (17.9%) Source: Council on Aging of Southwestern Ohio, 6/7/11 n= 69 Note: Information about secondary diagnoses were not collected until later in the process. These numbers are based on a total of 39 clients.
Our Initial Results: Sources: New England Journal of Medicine and Council on Aging of Southwestern Ohio, June 7, 2011. Note: This shows overall readmission and are not specific to the top 3 diagnoses; clients were admitted for one diagnosis and readmitted for another. Information for the 7.5% represents 4 out of 53 (# who completed CTI).
Our Initial Results: AMI, CHF & Pneumonia 30 Day Readmission at University Hospital Sources: CMS readmission report, and Council on Aging of Southwestern Ohio 6/7/11 Note: Information is based on clients who completed CTI (n=53) and were readmitted with the same diagnosis as their original admission (AMI=8, CHF=7, PNU=4).
Our Initial Results: 60.9% were discharged to a community setting Source: Council on Aging of Southwestern Ohio, 6/7/11: n=69 Note: N/A: includes individuals discharged from CTI and individuals who are still in the hospital.
Some Key learning: • Nursing Facilities can have higher readmit rates. • Hospitals have competing priorities and conflicting strategies • Nursing home diversion and care transitions can work together • The CMS grant opportunity was a huge help to rally partnerships and commitments
Cost model consideration examples • Fixed costs vs. variable costs • Partner costs • Target populations and volumes • Administrative and indirect costs • Productivity levels, turnover, training • Participation rate, drop-out rate • Partner costs • Margin • Projected impact and ROI
Closing thoughts • Care Transitions is a huge opportunity for Area Agencies on Aging • The window of opportunity to develop the product to meet the need is small • If you don’t step up, someone else will • Stepping stone for AAA’s position with ACO and Medical Home models