Download
1 / 62
620 likes | 685 Views
PROSTATITIS. underdiagnosed. מחלה שהאורולוגים שונאים. maltreated?. אז למה דווקא אני???!!. פרופ' אבי שטיין, מחלקה אורולוגית, מרכז רפואי כרמל. דלקת ערמונית. סיווג איבחון טיפול. טיפול בחימום דרך שפכה ( (TUMT ויעילותו כטיפול ב BPH. Prostatitis: A Major Clinical Problem.

E N D
PROSTATITIS underdiagnosed מחלה שהאורולוגים שונאים maltreated? אז למה דווקא אני???!! פרופ' אבי שטיין, מחלקה אורולוגית, מרכז רפואי כרמל
דלקת ערמונית • סיווג • איבחון • טיפול טיפול בחימום דרך שפכה ( (TUMT ויעילותו כטיפול ב BPH
Prostatitis: A Major Clinical Problem Incidence/prevalence: 4% -11% 8-12% of urologist office visits Life time prevalence 14.8% most common urological diagnosis in men <50 Quality of Life is dismal!
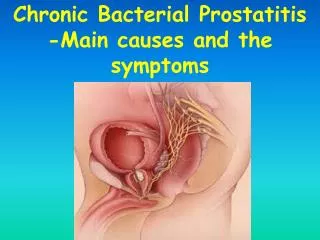
כיצד מתפתחת דלקת בערמונית?? • חיידקים מתנחלים בצינוריות של בלוטות ערמונית ויוצאים מטווח ההשפעה של אנטיביוטיקה או פקטורים של המערכת החיסונית ע"י יצירת אגרגטים (BIOFILMS) • הפרעות באספקת דם בערמונית על רקע טרומבוזיס (פקקת) בורידים הקטנים. זו כנראה אחת הסיבות ליעילות הנמוכה של טיפול אנטיביוטי בחולים עם פרוסטטיטיס כרונית. • תפקוד לא תקין של השריר החלק מסביב לבלוטות גורם להצטברות הנוזל. • בהמשך מופיעים ברקמת הערמונית חללים מלאים נוזל מזוהם ללא כל יכולת פינוי בעת שפיכה.
מיקרואורגניזם מחוללים • חיידקים גרם שליליים בד"כ ENTEROBACTERIA (קולי, פסיאודומונס וכו'- 90% מהמחוללים) בעקבות דלקת בדרכי השתן במנגנון של רפלוקס תוך-פרוסטטי. • חיידקים גרם חיוביים (קוקים למיניהם) • אנאירוביים • קלמידיה - האם דלקת שפכה קשור לדלקת ערמונית?? • פטריות • וירוסים • גורמים שלא ניתן לתרבת????
Classification: NIH Cat I: Acute Bacterial Prostatitis Cat II: Chronic Bacterial Prostatitis Cat III: Chronic Pelvic Pain Syndrome (CPPS) Cat IIIA: Inflammatory CPPS Cat IIIB: Non-inflammatory CPPS Cat IV: Asymptomatic Inflammatory Prostatitis (AIP) 90%
ACUTE PROSTATITIS SYMPTOMS Acute onset pain irritativeand obstructive voiding symptoms febrile illness. The patient typically complains of : • Urinary frequency, urgency, and dysuria. • Obstructive voiding complaints including hesitancy, poor interrupted stream, strangury, and even acute urinary retention are common. Tenesmus. • Perineal and suprapubic pain • Associated pain or discomfort of the external genitalia. • Significant systemic symptoms including fever, chills, malaise, nausea and vomiting, and even frank septicemia with hypotension Approximately 5% of patients with acute bacterialprostatitismay progress to chronic bacterialprostatitis (Cho et al., 2005
Acute bacterial prostatitis Supportive treatment Broad spectrum penicillins Aminoglycosides quinolones Transperineal approach?
CHRONIC PROSTATITIS DIAGNOSIS CLASSIC STAMEY 4 GLASS TEST bacterial Non- bacterial
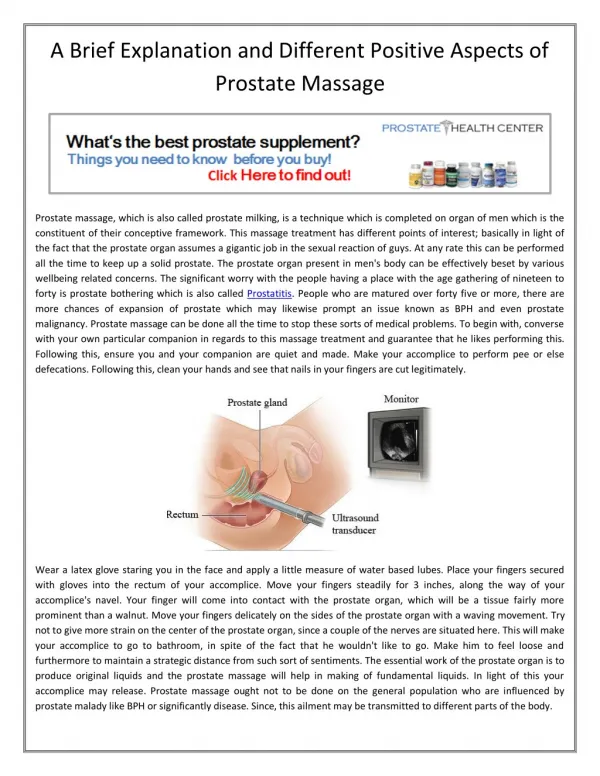
PRE-M POST-M Prostate massage
PROSTATITIS DIAGNOSIS Donna R. Coffman, MD Comparison of four-glass and two-glass premassage and postmassage test Nickel JC, Shoskes D, Wang Y, et al: How does the pre-massage and post-massage 2-glass test compare to the Meares-Stamey 4-glass test in men with chronicprostatitis/chronic pelvic pain syndrome? J Urol 176(1):119-124, 2006. The Premassage postmassage test (PPMT) may offer an adequate screening test as an alternative that is simpler, faster, and less expensive than the four-glass test.
CHRONIC BACTERIAL PROSTATITIS The prevalence of chronic bacterial prostatitis ranges from 5% to 15% of prostatitis cases 25-43 % of patients with a diagnostic glass test of prostatitis Have a history of chronic UTI
CP/CPPS CHRONICNON BACTERIAL PROSTATITIS cat III זו היא המחלה השכיחה הנקראת גם "כאב הראש של הערמונית"
Symptomatic WBC- negative postmassage urine CP/CPPS catIIIB Asymptomatic WBC- positive postmassage urine
CHRONIC NON-BACTERIAL PROSTATITIS • Inflammatory / Immunological • Endocrine • Neurological • Psychological • Role of normal prostate bacterial flora PATHOPHSIOLOGY
CHRONIC NON-BACTERIAL PROSTATITIS • Inflammatory / Immunological WBC in EPS or VB-3 Pro-inflammatory cytokines* (IFN,IL-6,IL-8, TNF) Anti-inflammatory cytokines* (IL-10) Autoimmunity PATHOPHSIOLOGY *soluble signaling molecules that are produced from leukocytes and other cell types. They serve as initiators and modulators of immune and inflammatory responses. There is poor correlation between these cytokines and the symptoms of prostatitis There may be a misinterpretation between cytokine levels obtained from seminal fluid and levels in serum obtained in other inflammatory conditions like RA, Sjorgen
CHRONIC NON-BACTERIAL PROSTATITIS • Endocrine Testosterone seems to have a protective anti-inflammatory effect. Recent animal studies demonstrate that inflammatory prostate presents with androgen insensitivity PATHOPHSIOLOGY
CHRONIC NON-BACTERIAL PROSTATITIS • Neurological The pain of CP may also be a result of “neurogenic inflammation” in the peripheral nervous system. PGE-2 is a known inflammatory marker. Inflammation decreases endorphine production. CP/CPPS patients present 4-6 times higher PGE levels and low endorphine levels compared to controls. After antibiotic treatment, the levels of PGE decresed while endorphine level increased. There seems to be a role for oxidative stress in the mechanism of prostatitis PATHOPHSIOLOGY
CHRONIC NON-BACTERIAL PROSTATITIS • Neurological (continued) Rat model spontaneous prostatitis: Degranulation of mast cells One of the products released from activated mast cells isnerve growth factor (NGF) one of the few factors that correlates with pain in CP/CPPS. NGF regulates the sensitivity of adult sensory neurons to capsaicin, which excites c-fibers. These C-fibers are sensory nerves associated with pain transmission and they also innervate mast cells. NGF is also a potent stimulator of mast cells and it can cause their degranulation. Released substances lead to “neurogenic inflammation” and then sensitize C-fibers PATHOPHSIOLOGY degranulation pain Mast cells NGF C fibers pain
CHRONIC NON-BACTERIAL PROSTATITIS • Psychological Psycological stress is a more frequent in patients with chronic non-bacterial prostatitis PATHOPHSIOLOGY
Classification: NIH Cat I: Acute Bacterial Prostatitis Cat II: Chronic Bacterial Prostatitis Cat III: Chronic Pelvic Pain Syndrome (CPPS) Cat IIIA: Inflammatory CPPS Cat IIIB: Non-inflammatory CPPS Cat IV: Asymptomatic Inflammatory Prostatitis (AIP)
תסמיני המחלה איזור חיץ הנקביים בתוך פי טבעת גב תחתון קצה הפין אשך ימין בסיס הפין אשך שמאל שק אשכים מרכז הפין מפשעה ימין מפשעה שמאל סביב פי טבעת לא ברשימה ללא כאב מתוך שאלונים שמילאו מאות חולים
Chronic Prostatitis Symptom Index (NIH-CPSI) Validation Process Pain Locations Severity Frequency Voiding Irritative Obstructive Quality of Life/Impact
Suggested Evaluation of a Man with CPPS cpps may be a great immitator *Mandatory History Physical examination, including digital rectal examination Urinalysis and urine culture Recommended Lower urinary tract localization test Symptom inventory or index (NIH-CPSI) Flow rate Residual urine determination Urine cytology Optional Semen analysis and cultureUrethral swab for culture Pressure flow studiesVideo urodynamics (including flow electromyography ( Cystoscopy Transrectal ultrasound Pelvic imaging (ultrasound, CT, MRI)Prostate-specific antigen)Nickel, 2002
Is prostatitis a premalignant lesion Prostate carcinogenesis and inflammation: emerging insights Patrick j. et al., Carcinogenesis 2005 26(7):1170-1181
Is prostatitis a premalignant lesion Review Nature Reviews Cancer 256-269 (2007) Inflammation in prostate carcinogenesis Angelo M. De Marzo, Elizabeth A. PlatzSiobhan Sutcliffe, Jianfeng Xu, Henrik Grönberg, Charles G. Drake, Yasutomo Nakai, William B. Isaacs & William G. Nelson
Treatment of chronic prostatitis ** Campbell’s urology **cannot be recommended as a monotherapy except perhaps in men with associated BPH.
Potential Therapies Antimicrobials (6-12 weeks in cat. II and trial of 2-4 weeks in cat. III) Alpha blockers ?? Muscle relaxants Anti-inflammatories Anti-depressants Other- finasteride, pentosan polysulfate, Phytotherapy, allopurinol, antioxidants Repetitive prostatic massage Biofeedback Heat treatment Intra-prostatic injections Transrectal shock waves
CPPS antibiotics??? • There is no real rationale for giving antibiotics to these patients as no bacteria were isolated. • Antibiotic therapy may benefit CPPS patients by three different mechanisms: • A strong placebo effect, the eradication suppression of non cultured microorganisms (Nickel et al, 2001a), • The independent anti-inflammatory effect of some antibiotics (Yoshimura et al, 1996; Galley et al, 1997). Is there a rationale to treat by antibiotics patients with cpps IIIa and IIIb who have been previously treated by antibiotics • Two multicenter randomized placebo-controlled studies have assessed the efficacy of 6 weeks of levofloxacin (Nickel et al, 2003b) and ciprofloxacin (Alexander et al, 2004) in men with CP/CPPS. In these trials the participants had chronic symptoms for a long duration (many years) and had been heavily treated (including treatment with antibiotics).. Antibiotics should not be prescribed for previously treated men with CP/CPPS of long duration.
Management Strategies Alpha blockers Alpha blockers
HYPERTHERMIA How to convey heat to the prostate: Transrectal (microwave) Transurethral (microwave) Interstitial (laser, Nanoparticles) Tuna (radiofrequency) Hifu (ultrasound) THOCHES - WERMUNG All treatments cause some degree of prostate tissue denaturation and if high temperatures are achieved, even tissue necrosis
TUMT • Thermotherapy 40-47 c • Cooled thermotherapy 80%
MICROWAVE - MECHANISM OF ACTION Microwaves produce electromagnetic radiation with oscillating electrical and magnetic fields. The design of the antenna seems to affect the heating pattern more than the wave frequency does Heat is produced while the microwaves are absorbed by the tissue. It arises mainly by electrical dipoles (water molecules) oscillating in the microwave field and electrical charge carriers (ions) moving back and forth in the field. These movements transfer energy to the tissue in form of heat.
LOCAL EFFECT OF TUMT • heating in excess of 45C is followed by coagulation necrosis • Histopathological effect of thermotherapy appears to be related to the induction of cell death • induced necrosis was shown to disrupt periurethral a-adrenergic receptors reflecting denervation of smooth muscle cells consisting with the increased urinary flow rate after TUMT • Recently, it was demonstrated that TUMT increased the sensory threshold (evoked by electrical stimulation) in the posterior urethra by 30%, resulting in the reduction of irritativesymptoms
60 Heating point center Heat Distribution For BPH: 55 to 60°C For Prostatitis: 47° C
Heating Point Balloon Heating Point Center
The urethral heatingSystem • Microwave energy source • Computerized console • Multi-use Applicator Thermaspec consists of:
Applicator Assembly Balloon Channel Balloon Inflate Applicator Balloon Thermocouple Urinate Cannel Heating Point Marker