Download
1 / 12
120 likes | 449 Views
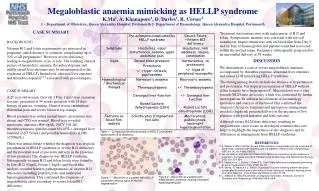
Case Summary. 29 yo M with HIV (CD4 25, VL 48,000), TB (lung, bone marrow), HBeAg negative chronic HBV infection, schistosomiasis and cryptococcal meningitis presenting with jaundice about 3 months after starting AZT/3TC/EFV.

E N D
Case Summary • 29 yo M with HIV (CD4 25, VL 48,000), TB (lung, bone marrow), HBeAg negative chronic HBV infection, schistosomiasis and cryptococcal meningitis presenting with jaundice about 3 months after starting AZT/3TC/EFV. • Exam notable for icterus, hepatosplenomegaly and no signs of chronic liver disease. • He has elevated total bilirubin (conjugated and unconjugated) and ALT and evidence of hepatic synthetic dysfunction. CXR: improving infiltrates on TB therapy. • A liver biopsy done just after starting ARVs, but before the development of jaundice, showed mild inflammatory changes and steatosis, but no evidence of granuloma or malignancy.
Differential Diagnosis • Drug-induced liver injury • Malignancy • Immune reconstitution syndrome • Other infections • Fungal • Parasitic • Viral • Hepatitis B
Drug-induced liver injury • Possible causes: • ARVs, particularly EFV • Antituberculous therapy, either INH or rifampicin • However, now ~4-5 months into ATT • Fluconazole can occasionally cause liver injury. • Was he on this drug at the time of the jaundice? • Bactrim. • Was he on this drug at the time of the jaundice? • ? Any use of traditional medicines or alcohol
Malignancy • Kaposi’s sarcoma • No evidence of cutaneous disease or other sites of visceral involvement • Lymphoma • No adenopathy • No paraneoplastic phenomenon, such as hypercalcemia • Hepatocellular carcinoma • Metastatic carcinoma • No known primary site
Immune reconstitution Syndrome • TB • No evidence of TB IRIS elsewhere • Not told that he is having any fevers, chills, sweats • No significant adenopathy on exam or CXR • Pulmonary infiltrates are improving • Pancytopenia—evidence of myelophthsis on peripheral smear? • HBV • Will come back to this possibility • Other: MAC, cryptococcus
Other infections • Schistosomiasis • Detected on rectal biopsy (not told why it was done) • S. mansoni and japonicum are the usual causes of liver disease • S. mansoni present in Africa • Adult worms live in the mesenteric vessels of the colon in permanent copulation • Eggs travel hematogenously to the liver and other sites • In the liver, eggs lodge in the presinusoidal spaces of the portal vein and elicit a granulomatous fibrosing reaction • Secondary portal hypertension ensues, leading to splenomegaly, ascites, varices • One would not expect rapidly deteriorating liver function tests or hepatic dysfunction in chronic schistosomiasis • Patient did not have symptoms of acute schistosomiasis (Katayama fever) or signs of chronic portal hypertension • No evidence of granulomas or fibrosis on recent liver bx
Other infections • CMV • CMV can cause acute hepatitis • May be associated with a mononucleosis-like syndrome, with atypical lymphocytosis • CMV IgM positive, but this can be unreliable unless done in an experienced lab • CMV antigenemia or PCR is usually more reliable • Would check CMV IgG • Cryptococcus • Look for evidence of recurrent cryptococcus in the CNS or blood • Bacterial infections: Syphilis, Bartonella (peliosis hepatis), Salmonella, Listeria
Viral hepatitis • HAV • HCV • HDV • CMV • EBV • HSV
HBV • HBeAg negative • May be due to long-standing infection, development of pre-core mutant • May be more aggressive • Check HBV DNA
HBV Flare • HBV Resistance • 25%/year of 3TC monotherapy • Has only been on 3TC for 3-4 months • Discontinuation of 3TC • Patient had been receiving DOT in hospital • Review adherence • Fibrosing cholestatic hepatitis • HBV IRIS
What would I do? (1) • Check abdominal U/S: • ? Adenopathy, obstruction • Monitor PT, platelets, albumin closely • Give oral vitamin K • Check serologies for HAV, HDV, HCV, EBV, CMV IgG and PCR, RPR • Check HBV DNA • Hold antituberculous therapy, fluconazole, bactrim
What would I do? (2) • Liver biopsy • If presence of eosinophils, suggests drug-induced liver injury • Stain for HBV. Look for inflammation to suggest HBV flare • Look for fibrosing cholestatic hepatitis • If liver biopsy shows HBV is the main problem, then would add tenofovir, would not add steroids