Download
1 / 41
420 likes | 503 Views
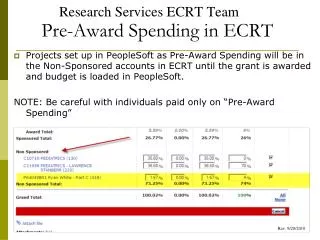
What can we learn from NHA and HIV spending accounts?. Jose Antonio Izazola. $17.4. 17.5. $17,0. $15.9. $15.6. 15.0. $14,3. $14.4. $12,8. 12.5. $11.4. Signing of Decleration of. 10.0. $8.9. Commitment on HIV/AIDS, UNGASS. US$ billion. $09,9. $8.3. 7.5. HIP+. $6.1.

E N D
What can we learn from NHA and HIV spending accounts? Jose Antonio Izazola
$17.4 17.5 $17,0 $15.9 $15.6 15.0 $14,3 $14.4 $12,8 12.5 $11.4 Signing of Decleration of 10.0 $8.9 Commitment on HIV/AIDS, UNGASS US$ billion $09,9 $8.3 7.5 HIP+ $6.1 World Bank UNITAID MAP launch $5.0 5.0 $3.2 UN AIDS Gates PEPFAR Foundation 2.5 $0.9 $0.5 $0.5 The Global Fund $0.3 $1.6 $1.4 0.0 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 TOTAL annual resources available for AIDS in low and middle income countries, 1996-2009
Resources Available for AIDS from All Sources, 2009 $15.9 billion available in 2009 for HIV in low and middle income countries 16.0 Foundations (4%) UN and other 12.0 Multilateral (4%) Contribution to GFATM (11%) USD billions 8.0 Bilateral contributions (37%) 4.0 Domestic-public and private- (44%) 0.0
Expenditures from international sources as percentage of total HIV spending
National Aids Spending Assessment Principles: NASA is inspired from broader social accounting systems. Its methods rest mainly on principles sustained in the System of Health Accounts (SHA) – National Health Accounts (NHA). National Aids Spending Assessment System of National Accounts System of Health Accounts & National Health Accounts National Health Sub Accounts (HIV, Malaria, etc)
National Aids Spending Assessment NASA: Social Mitigation Health NASA does tracks resources of health services, social mitigation, education, labour, justice and other sectors to embody the multi-sectoral response. HIV Education Labour Human Rights
NASA and NHA NASA divergence with NHA: NASA does not confine itself to health expenditures and the sector boundary overlaps with other sub-accounts (i.e.: Reproductive Health, Education…) NASA tracks health and non health related HIV expenditures e.g. STI HIV health related e.g. Malaria, TB, hepatitis, etc
HIV Spending - Defining Boundaries - NASA follows the space and time boundaries of national health accounts. - NHA Health Spending Health Accountants - NASA HIV spending NASA resource tracking team
Both NASA and NHA aim to… • Address critical policy questions (for both national and international stakeholders) i.e. • “what are we getting for the money?” • What matters is not only how much is invested but… • How funds are invested • Whether or not funds are reaching intended targets • Serve as advocacy and monitoring tools, supporting evidenced-based policy processes • e.g. informing resource allocation decision-making • Provide country comparable data
Coordination complies with the UNAIDS “three ones principle” • For coordination of national HIV/AIDS responses • ONE agreed HIV/AIDS action framework that provides the basis for coordinating the work of all partners, • ONE National AIDS coordinating authority, with a broad-based multisectoral mandate, and • ONE agreed country level monitoring and evaluation system.
NASA: resource tracking $M F Agent (Ministry of Finance) Clinic Source MoH (Ministry of Health) Provider (Ambulatory Center) Beneficiary Population Aids Spending Categories
Financial and Expenditure Flows Consumption Flow Financial Flow
The agents’ triangulation = Financing Sources & Financing Agents Providers & Production Factors Financing Provision = = Consumption Aids Spending Categories & Beneficiary Populations
NAP and NASA (US $ '000) 25,000 21,294 20,000 15,000 10,000 8,346 7,037 5,110 5,000 2,976 1,215 1,626 960 466 269 418 - - Prevention Treatment, Care Advocacy, Policy, Leadership and Strategic info, M Finance and and Support Legal reform management & E resource mob NAP NASA 2007 Planned vs. executed - Nepal 2007
Total HIV spending GR 2010, last year reported - Top 15 Globally 900 Millions 800 700 600 500 International USD Public 400 300 200 100 0 India 2009 Brazil 2008 China 2009 Kenya 2009 Malawi 2009 Nigeria 2008 Mexico 2009 Uganda 2008 Rwanda 2008 Thailand 2009 Argentina 2008 Colombia 2009 Botswana 2008 Mozambique 2008 Russian Federation 2008 Last year reported Top spenders – Last year reported
Total HIV spending per capita GR 2010, last year reported - Top 15 Globally 200 180 160 140 120 International per capita USD 100 Public per capita 80 60 40 20 0 Chile 2008 Cuba 2009 Belize 2009 Kenya 2009 Gabon 2009 Malawi 2009 Uganda 2008 Lesotho 2008 Rwanda 2008 Argentina 2008 Botswana 2008 Swaziland 2007 El Salvador 2008 Mozambique 2008 Russian Federation 2008 Last year reported Top spenders per capita – Last year reported
100% 90% 80% 70% 60% International 50% Public 40% 30% 20% 10% 0% Low income Lower middle income Upper middle income (n = 29) (n = 25) (n = 15) Funding sources by income level, Last year reported
35 30 25 PRIVATE 20 US$ million PUBLIC 15 INTERNATIONAL 10 5 0 2007 2008 Total HIV and AIDS Expenditure, Senegal 2007-2008
Other multilateral, Foundations and 230,264 international NGOs, 531,441 UN agencies, 741,153 Bilateral, 10,223,460 GFATM, 7,640,509 International HIV and AIDS Expenditure, Senegal 2007-2008
Profiles of Spending by Beneficiaries in Sierra Leone 2007 100% Other populations 90% 80% Non-targeted interventions 70% General population 60% Children and Youth in 50% school 40% Orphans and vulnerable 30% children (OVC) MARP's 20% 10% PLWHA 0% Public Funds Bilateral Funds Multilateral Funds
Spending by Providers Ministry of Health Multilateral Hospitals, (including. agencies , 82,151 , 0% NAPs/NACPs) , 430,696 , 2% 2,247,182 , 13% Other Ministry, 5,785 , 0% NGO, INGOs, CBO, 14,895,801 , 85% Providers of Services (PS) NASA - Nepal 2007
BP.99 Specific BP.01 People Expenditure by BP targeted living with HIV US $ 17,661,653 populations not (regardless of elsewhere having a classified (n.e.c.) medical/clinical 3% diagnosis of AIDS) 12% BP.05 Non- targeted interventions 27% BP.02 Most at risk populations 30% BP.04 General population 9% BP.03 Other key and accessible populations 19% Beneficiaries Population - Nepal 2007
Allocation of resources by programmatic area by type of epidemic 100% 90% 80% Research 70% Enabling Environment Social Protection and Social Services excluding 60% Orphans and Vulnerable Children Human resources 50% Program Management and Administration Strengthening 40% Orphans and Vulnerable Children Care and Treatment 30% Prevention 20% 10% 0% C G L (n = 41) (n = 30) (n = 20)
2,500 Millions 2,000 Research Enabling Environment Social Protection and Social Services excluding 1,500 Orphans and Vulnerable Children Human resources Program Management and Administration Strengthening 1,000 Orphans and Vulnerable Children Care and Treatment Prevention 500 0 International Public Allocation of resources by programmatic area by Funding Source, Sub-Saharan Africa last year available USD
100% 90% 80% 70% 60% 50% International Public 40% 30% 20% 10% 0% Oceania East Asia Caribbean North America North Africa Middle East and South and South- East Asia Central and South America Sub-Saharan Africa Eastern Europe and Central Asia Western and Central Europe (n = 1) (n = 3) (n = 1) (n = 3) (n = 1) (n = 11) (n = 11) (n = 11) (n = 11) (n = 21) MARPS Funding sources by UNAIDS regions, Last year reported
HIV spending by broad category and detailed prevention distribution. Botswana, 2007. (Million USD)
Spending in programs specifically directed to the populations most at risk for HIV as a percentage of total prevention
A health system comprises all organizations, institutions and resources devoted to producing actions whose primary intent is to improve health. Most national health systems include public, private, traditional and informal sectors. The four essential functions of a health system have been defined as service provision, resource generation, financing and stewardship. Health Systems
HIV/AIDS Spending on HSS & General Health: Zambia 2007, 15% of THAE Swaziland, 11% of THAE
The categories included as HSS or for general health spending were: • Blood safety • Safe medical injections • Universal precautions • Opportunistic infection (OI) prophylaxis • Specific HIV-related laboratory monitoring • Opportunistic infections' (OI) treatment (??) • Patient transport and emergency rescue • OVC Basic health care • Monitoring and evaluation • Operations research • Drug supply systems • Information technology • Upgrading and construction of infrastructure • Upgrading laboratory infrastructure and new equipment • Construction of new health centres • Upgrading and construction of infrastructure n.e.c • Home-based care • Human Resources and Training • Research, • Capacity strengthening 34
Total Expenditures per capita by income level and type of expenditures, 2006 100 80 60 % of Total Expenditures 40 20 0 Low Lower middle Upper middle High nonOECD High OECD Health System Strengthening Health Non Health Number of Countries: Low (17), Lower middle (19), Upper middle (14), High nonOECD (2), High OECD (3)
Total Expenditures by region and type of expenditures, 2006 Caribbean East Asia Eastern Europe & Central Asia Latin America MENA Oceania South & South East Asia Sub-Saharan Africa Western and Central Europe 0 20 40 60 80 100 % of Total Expenditures Health System Strengthening Health Non Health Number of countiries: Sub-Saharan Africa(17), Latin America(12), Eastern Europe & Central Asia(10), South & South East Asia(5), Caribbean(4), East Asia(2), MENA(3), Oceania (1), Western and Central Europe(1)
Total Expenditures by region and type of expenditures, 2006 Caribbean East Asia Eastern Europe & Central Asia Latin America MENA Oceania South & South East Asia Sub-Saharan Africa Western and Central Europe 0 20 40 60 80 100 % of Total Expenditures Health System Strengthening Health Non Health Number of countiries: Sub-Saharan Africa(17), Latin America(12), Eastern Europe & Central Asia(10), South & South East Asia(5), Caribbean(4), East Asia(2), MENA(3), Oceania (1), Western and Central Europe(1) HSS or general health spending SSA, 2006
Use of NASA/policy implications • Improved financial information system for quality and accuracy of data • Improving implementers reporting and alignment as well as harmonisation of classification • Institutionalising NASA as a part of national M&E system • National capacity and EDPs role questioned
Use of NASA//policy implications • Useful in assessing the expenditures and getting a broad picture of resource availability in the reporting period. • Used extensively in reports at country and global level. Highlighting resource gaps • Referred during Global Fund Proposal development.