Download
1 / 40
430 likes | 770 Views
Hospital Management of Decompensated Heart Failure Wilson S. Colucci, MD Chief, Cardiovascular Medicine. Acute Heart Failure Syndromes. Acute (i.e., new) onset of HF in patient without prior episodes or history of HF (e.g., acute MI, myocarditis)

E N D
Hospital Management ofDecompensated Heart FailureWilson S. Colucci, MDChief, Cardiovascular Medicine
Acute Heart Failure Syndromes Acute (i.e., new) onset of HF in patient without prior episodes or history of HF (e.g., acute MI, myocarditis) Worsening (“decompensation”) of existing chronic, “compensated” heart failure Persistently decompensated HF despite optimal medical management (often referred to as advanced or end-stage HF)
AHFS • About 900,000 admissions per year • Average LOS 6-7 days • $23 billion annual costs • Affects most patients with chronic HF
Admissions for Heart Failure: Frequent Flyers Initial Admission 21% • Rates of readmission • 2% in 2 days • 20+% in 30 days • 50% in 6 months Readmission 79%
Causes of Readmission for HF Rx Noncompliance 24% Diet Noncompliance 24% 16% Inappropriate Rx 17% Other 19% Failure to Seek Care HFSA Research 2000
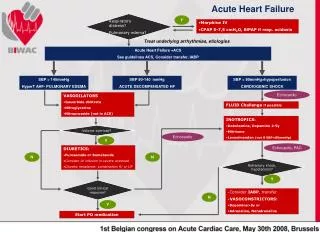
Overall Goals in Management of AHFS Immediate relief of symptoms and hemodynamic stabilization Identification and correction of underlying / precipitating factors Optimize fluid status (optimal weight, renal function, edema) Establishment of effective ambulatory regimen prior to discharge Discharge planning and follow-up
Precipitants of AHFS Diet indiscretion Medication non-compliance Uncontrolled hypertension Myocardial ischemia/infarction Cardiac arrhythmia (rapid heart beats, loss of atrial kicks) Exacerbation of COPD Medications (NSAID, glitazones, diltiazem verapamil)
Patient: W.C. • 67 year old man, ischemic CMP admitted with progressive DOE and fatigue • HR 98, tachypnea, BP 100/84, CVP 16 cm, bibasilar rales, 3+ edema to knees, cold feet • Labs: BUN 50, creat 2.5, BNP 1,500
Volume Status Dry Wet Warm A - Normal B Perfusion D C Cold Hemodynamic Profiles Dyspnea Rales CVP Edema Cold extremities Hypotension Narrow PP Renal insuff.
Acute HF: Clinical Signs • Intracardiac Filling Pressures • orthopnea, dyspnea on exertion • rales, jugular vein distention • bedside Valsalva maneuver • chest x-ray • Adequacy of Perfusion • narrow pulse pressure • cool extremities • mental obtundation • renal insufficiency, oliguria
LV Failure Easily Missed on Exam and/or CXR • By exam - rales, edema, and JVD often absent (e.g., 42% in Stevenson et al., JAMA 1989;261:884) • By CXR – congestion often absent (e.g., 27% had no congestion and 41% had minimal congestion in Mahdyoon et al., AJC 1989)
PA Catheter • Gold standard, but usually/often not needed • Adds little to management of uncomplicated case • ESCAPE Trial • Indicated/valuable in patient with known LV failure if: • Suspected low output / hypoperfusion • Unclear volume status • Ischemia, renal insufficiency, ARDS • Poor / unclear response to IV therapy / to optimize oral therapy
Predictors of In-Hospital Mortality • Three best predictors of mortality in hospitalized patients • BUN > 43 mg/dL • SBP < 115 m Hg • Creatinine > 2.75 mg/dL • But, information mainly retrospective from registry data (e.g., ADHERE Registry) • Therefore, not that useful in individual patient, but identifies patients to worry about Fonarow GC et al. JAMA 2005;293:572-80.
Diuretics can worsen renal function in HF ? Inc Morbidity and Mortality Diuretic Therapy Decreased preload Diuretic & Natriuretic Resistance Neurohormonal Activation Diminished Renal blood flow Worse renal function
Diuretics can improve renal function in HF 1.4 1.1 GFR (ml/min) 0.8 0.5 0 6 12 19 25 0 CVP, mm Hg 0 2 4 6 8 Firth et al Lancet 5/7/88
Intensification of diuretic regimen When diuresis is inadequate to relieve congestion, as evidenced by clinical evaluation, the diuretic regimen should be intensified, using either: 1) higher doses of loop diuretics; 2) addition of a second diuretic (e.g. metolazone, spironolactone, or chlorothiazide); or 3) continuous infusion of a loop diuretic (Level of Evidence: C)
NIH “Dose” Trial: How to Diurese To evaluate the safety and efficacy of various initial strategies of furosemide therapy in patients with ADHF • Route • Q12 hours bolus • Continuous infusion • Dose • Low intensification (1 x oral dose) • High intensification (2.5 x oral dose)
Acute Heart Failure (1 symptom AND 1 sign) <24 hours after admission 2x2 factorial randomization Low Dose (1 x oral) Q12 IV bolus Low Dose (1 x oral) Continuous infusion High Dose (2.5 x oral) Q12 IV bolus High Dose (2.5 x oral) Continuous infusion 48 hours 1) Change to oral diuretics 2) continue current strategy 3) 50% increase in dose 72 hours Co-primary endpoints 60 days Clinical endpoints Dose: Study Design
Conclusions • There was no statistically significant difference in global symptom relief or change in renal function at 72 hours for either: • Q12 bolus vs. Continuous infusion • Low intensification vs. High intensification
Conclusions (2) • There was no evidence of benefit for continuous infusion compared to Q12 hour bolus on any secondary endpoint • Despite transient changes in renal function, there was no evidence for higher risk of clinical events at 60 days associated with the high intensification strategy • High intensification (2.5 x oral dose) was associated with trends towards greater improvement in multiple domains: • Symptom relief (global assessment and dyspnea) • Weight loss and net volume loss • Proportion free from signs of congestion • Reduction in NT-proBNP
Diuretic Resistance: Other Approaches to Consider Addition of inotrope (e.g., dobutamine) and / or vasodilator (e.g., nesiritide), or inodilator (e.g., milrinone) to improve cardiac output, and hopefullly, renal perfusion Addition of low-dose dopamine to increase renal perfusion Vasopressin antagonists if hyponatremic (tolvaptan,i.v., lixivaptan, p.o.) Ultrafiltration
Pre- and Post-Discharge Management Stable weight (for at least 2 days) on stable doses of oral diuretics Pre-discharge education (i.e., diet, weight, medications, activity level and what to do when problems arise) Discharge planning with CMP nurse Follow-up visits with CMP Clinic and primary physicians, etc
Dry Wet Warm A - Normal B D C Cold Patient: Not diuresing • 67 year old man, ischemic CMP admitted with progressive DOE and fatigue • Modest response to diuretics, still very sob • BP 100/84, HR 98, bibasilar rales, pedal edema, cool feet • Labs: BUN 50, creat 2.5, BNP 1,500 • Poor response to continuous infusion furosemide • PA catheter: RA 17, PCWP 34, CO 2.7 (CI 1.6), SVR 1870 • Which drug would you use next? 1. Dobutamine 2. Dopamine 3. Nitroglycerin 4. Milrinone 5. Nitroprusside 6. Nesiritide
“Typical” management of patients with ADHF who fail continuous furosemide 50% Discharge 76% Continuous IV Lasix 50% No/Partial Response to Lasix Bolus
“Typical” management of patients with ADHF who fail continuous furosemide 50% 90% 80% Discharge Discharge Discharge 76% 20% 10% Continuous IV Lasix Natrecor Die/Mech Assist/Tx 20% Inotropes 30% Discharge Other 50% (750,000) 90% Inotropes 80% Die/Mech Assist/Tx 10% 4% No/Partial Response to Lasix Bolus Discharge Natrecor 20% Discharge 95% Inotropes 18% 70% Inotropes 5% Die/Mech Assist/Tx Discharge 30% 2% Die/Mech Assist/Tx Die/Mech Assist/Tx
Agonist 1AR Gs Ca++ ACase cAMP PKA Inotropes: Beta-Agonists
Dobutamine: beta1-Adrenergic Agonist • Stimulates cAMP • Inotrope, weak vasodilator • Titrated to cardiac index • Side effects: Tachycardia, arrhythmias, ischemia • Hypo-responsiveness • Variable inotropic response, needs to be titrated Colucci et al., Circulation 1986;73:III175
Dobutamine vs. Dopamine Dob: 2.5-10 g/kg/min Dopa: 2-8 g/kg/min CI CI CI Leier et al., Circulation 1978
Agonist 1AR Gs Ca++ ACase cAMP PKA PDE3 AMP PDEinh. Inotropes: PDE Inhibitors
Milrinone: PDE Inhibitor • Inhibits phosphodiesterase, thereby increasing cAMP in myocardium and vasculature • Potent inotrope • Potent vasodilator • Side effects similar to dobutamine (tachycardia, arrhythmias, ischemia) plus hypotension • Simplified dosing
Hemodynamic effect of arterial dilation BP = CO X SVR Normal SVR CO BP HF SVR CO BP
Venous Arterial Vasodilator Classification Venous Nitrates Mixed Nitroprusside Nesiritide ACEI ARBs Arterial Hydralazine
Nitroprusside • Very potent, balanced, direct-acting vasodilator • Very rapid action • Requires central monitoring • Effects highly variable patient-to-patient • Cyanide and thiocyanide toxicity • Rebound after withdrawal
2Na+ -- CN CN CN Fe -NO CN CN Nitroprusside: Toxicity Renal dysfunction Thiocyanate toxicity Liver dysfunction Cyanide toxicity
Hemodynamic Effects of Hydralazine and Isosorbide Dinitrate HZ + ISO HZ Stroke Volume Baseline Pulmonary Capillary wedge Pressure As per Chatterjee K, Parmley WW, Massie B, et al. Circulation 1976; 54: 879-883.
Endothelium NO-donating Drugs ANP BNP (nesiritide) NO NP Receptor Particulate Guanylate Cyclase Soluble Guanylate cyclase cGMP Vasodilation NO-mediated vasodilation: Natriuretic peptides Vascular Smooth Muscle Cell
PCWP (mm Hg) 35 placebo 30 0.015 µg/kg/min * 25 * * 0.03 µg/kg/min 20 15 CI (L/min/m2) 2.5 2 1.5 BL 1.5 3 4.5 6 Colucci, et al. NEJM 2000; 343:246-53 Nesiritide: A gentler nitroprusside • Direct-acting balanced vasodilator • Less potent and rapid than NTP • But, does not require central monitoring and no direct toxicity • However, not a diuretic • Dose-related hypotension • Concerns about renal effects • Concerns about adverse outcomes • ASCEND Trial – neutral outcomes • Use as needed for symptoms and hemodynamics, not outcomes Time (hours)
Updated Guide to Initial Therapy CO Low Low Low PCWP High High High SVR High Normal Low BNPBNP Dob SNP SNP Dopa TNG Dob +/- VD MilrinoneMilrinone Modified from Stevenson and Colucci, Cardiovascular Therapeutics