Download
1 / 13
140 likes | 394 Views
The Use of Goldfinger to Facilitate Glidescope Tracheal Intubation in a Morbidly Obese Patient. Ahed Zeidan, MD Sultan Al-Temyatt MD Department of Anesthesiology Department of Bariatric Surgery Badana Clinic Procare Riaya Hospital Al-khobar Kingdom of Saudi Arabia

E N D
The Use of Goldfinger to Facilitate Glidescope Tracheal Intubation in a Morbidly Obese Patient Ahed Zeidan, MD Sultan Al-Temyatt MD Department of Anesthesiology Department of Bariatric Surgery Badana Clinic Procare Riaya Hospital Al-khobar Kingdom of Saudi Arabia Anesthesia & Analgesia March 2011 • Volume 112 • Number 3
A common factor preventing successful tracheal intubation is the inability to see the vocal cords during direct laryngoscopy. Videolaryngoscopy using any of a variety of recently described instruments usually provides excellent glottic visualization, but directing an endotracheal tube (ETT) through the vocal cords may be difficult.
The use of stylets, guides, or bougies frequently assists in directing the tip of the ETT. • However, these devices do not allow manual control of the tip of the ETT. • The Goldfinger (Ethicon Endo Surgery, Johnson & Johnson, Cincinnati, OH), a stylet device used in the placement of the gastric band for bariatric surgery, has the option of maneuverability of its distal tip.
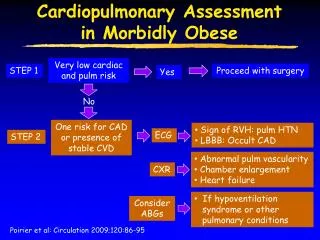
Case report • An obese 20-year-old, otherwise healthy but morbidly obese woman weighing 129 kg, and whose height was 169 cm (body mass index [BMI] 45 kg/m2), presented for laparoscopic Roux-enygastric bypass surgery. • On examination she had Mallampati class II, upper lip bite test class I, a thyromental distance 6 cm, but good mouth opening.
After premedication (midazolam 3 mg, glycopyrrolate 0.2 mg) and administration of oxygen, anesthesia was induced using propofol, fentanyl, and succinylcholine. • The patient’s head was in the sniffing position. • Direct laryngoscopy revealed Cormack–Lehane grade III view, and we were not able to obtain a view of the glottis sufficient to intubate the trachea.
A Glidescope videolaryngoscope provided a good glottic view but 3 more attempts using Schroder, malleable, and J-shape stylets respectively failed to advance the ETT through the vocal cords. • Our surgeon, recognizing our need for better ETT tip manipulation, suggested a Goldfinger device for this purpose.
After additional propofol and succinylcholine, the stylet of the Goldfinge was inserted into a 7.0- mm internal diameter configuring the ETT with a 90° bend. • While using the Glidescope videolaryngoscope with the ETT tip facing the trachea and rotating the Goldfinger counterclockwise to bend its tip 70° to 80° together with the ETT, a partial passage of the ETT tip through the vocal cords was provided.
Anterior advancement of the ETT in combination with a 45° downward relaxation of the Goldfinger tip was enough to achieve the passage of the ETT through the vocal cord. • Removal of the Goldfinger stylet was easy and uneventful, whereupon auscultation and capnography confirmed tracheal placement of the ETT.
The Goldfinger stylet consists of 3 parts: a flexible tip, a metallic body, and a handle providing maneuverability of its distal tip. • The tip of the Goldfinger can flex 90° in the vertical axis by simple rotation of its handle. • The tip of the Goldfinger can be set at varying degrees between neutral position and 90°.
Tip rigidity is angle dependent. • When bent 90°the tip is rigid; thus a slight relaxation of its curvature gives the tip a soft flexible property, making its removal easy. • Alternatively, Endotrol (Nellcor, Pleasanton, CA) is a modified tracheal tube with available directional tip control via a ring loop. • It is designed for use in patients requiring directional tip control of the tracheal tube.
Thank you for your attention