Download
1 / 18
190 likes | 1.3k Views
Pain Relief in Labor. Khalid A. Yarouf. . www.4MedStudents.com. Pain pathways during labor. Pain is sensation of discomfort resulting from stimulation of specialized nerve endings.

E N D
Pain Relief in Labor Khalid A. Yarouf . www.4MedStudents.com
Pain pathways during labor • Pain is sensation of discomfort resulting from stimulation of specialized nerve endings. • During labor, pain sensation is relayed to the spinal cord from T10, L1, S1-S4. These sensory fibers make synaptic connections in dorsal horn of spinal cord with cells that provide axons that make up the spinothalamic tract.
Early 1st stage: before fetal head reaches zero station, pain impulses arise primarily from uterus via visceral afferents enter spinal cord at T10-L1. • Late 1st stage & 2nd stage: pain impulses arise from uterus, pelvic structures, vagina, & perineum. • 3rd stage of labor is usually well tolerated with spontaneous placental delivery.
Analgesia • Psychoprophylaxis & physical analgesia • “Nature childbirth” (e.g. Lamaze prenatal classes) whereby informed mother utilizes relaxation techniques to stimulate descending inhibitory pathways. • Whirlpool baths, transcutaneous nerve stimulation & acupuncture inhibit nociceptive impulses & reduce pain propagating muscle tension. • Especially effective in early stages of labor.
Con’t Analgesia • Systemic medications • Narcotics: • Although narcotics provide both analgesic & sedation, their S.E are: • Maternal: Orthostatic hypotension, nausea, vomiting. • Fetal: ↓ beat-to-beat variability of FHR. • Neonatal: respiratory depression Rx: Naloxone (Narcan).
Con’t Analgesia Meperidine (Demerol or Pethidine): • Best use in early stages of labor, less effective once labor is well established. • If IV (25-50 mg) peak effect = 7-8 min. Duration = 1.3-3 hrs. • If IM (50-100 mg) peak effect = 2-4 hrs.
Con’t Analgesia Fentanyl: • Most frequently used for parturient in active labor. • Administered in 2-3 divided doses of 25 μg given 5 min apart. • Peak analgesic effect = 5-6 min after each IV injection. Duration = 30-60 min.
Con’t Analgesia • Sedative-Tranquillizers • These agents given in combination with a narcotic. • The phenothiazine –Promethazine (Phenergan)- 25 mg IM or 12.5 mg IV. • Relieves anxiety, controls nausea & vomiting, ↓ narcotic requirements during labor.
Con’t Analgesia • Inhalational analgesia (NO) • Provides partial pain relief during labor as well as @ delivery. • 50% NO in O2. It’s administered with a mask / mouthpiece in a manner such that the parturient remains awake, cooperative & in control of her airway to prevent pulmonary aspiration of gastric contents. • Does not prolong labor or interfere with uterine contractions but administration > 20 minutes may result in neonatal depression. • A/w < risk of neonatal depression when compared with narcotics.
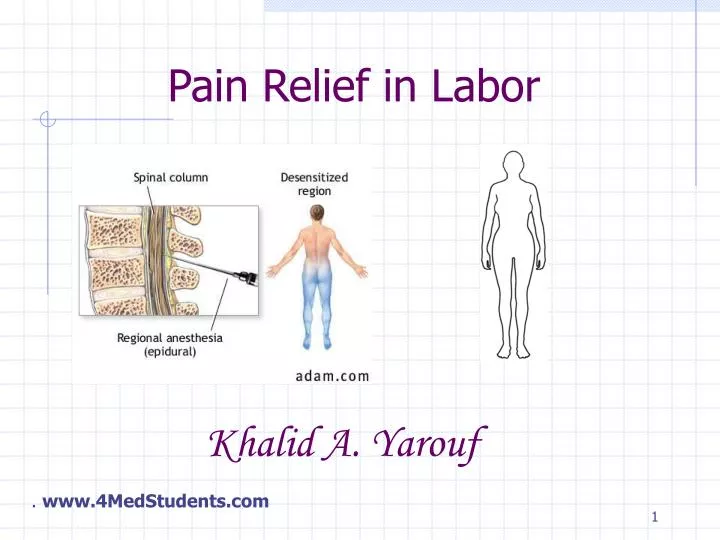
Anesthesia (Regional anesthesia) • Peripheral nerve block: • Local infiltration for episiotomy (Lidocaine). • Pudendal block. • Central nerve block: • Epidural anesthesia. • Spinal (subarachnoid) block.
Con’t Anesthesia Pudendal block: • Administered shortly before delivery to anesthetize pudendal nerve. • Insert needle aspirate with syringe to check for absence of blood inject 1% Lidocaine on each side. • Analgesia produced in lower birth canal & perineum provides maternal comfort for low forceps delivery & episiotomy. • Advantages: easy to administer, not a/w maternal hypotension/ fetal distress. • Disadvantage: incomplete analgesia @ time of delivery, since pain of uterine contraction is unaffected.
Con’t Anesthesia Epidural anesthesia: • Most commonly used technique for both labor & delivery. • 19 gauge indwelling catheter inserted into lumbar epidural space @ L3-4.
Con’t Anesthesia • Does not prolong 1st stage, but may reduce maternal expulsive efforts, therefore usually used in earlier stages of labor (<4 cm).
Con’t Anesthesia • During early labor, analgesia is established with Fentanyl + small dose of Bupivacaine (Marcaine). • Epidural opiate (Fentanyl) provides effective analgesia for visceral pain arising from uterus. • Local anesthetic (Bupivacaine) relieves somatic pain of labor, which begins once fetal head engages pelvis (at zero station). • If perineal anesthesia (for muscle relaxation) is needed to facilitate difficult vaginal delivery 2% Lidocaine (Xylocaine).
Con’t Anesthesia • Certain precaution must be taken: • Preload mother with 5 mL IV fluid to prevent assess pt for evidence of spinal shock (e.g. rapid loss of sensory function). • If no spinal shock give another 5 mL assess for signs of intravascular injection (dizziness, tinnitus) if nothing happens, rest of dose is given @ rate of 5 mL/min. • Cx: inadvertent total spinal with cardiovascular collapse & resp arrest, intravascular injection with seizures, post-ictal depression & possible cardiac arrest.
Con’t Anesthesia Spinal (subarachnoid) block: • Injection of local anesthetic (Tatracaine, Bupivacaine, or Lidocaine) into subarachnoid space thru a spinal needle placed in L3-4 interspace. • Fastest onset. • Least drug exposure for fetus because small dose required. • Beware of rapid hypotension & preload mother with 1000 mL IV fluid.
Anesthesia (General) • Not used to vaginal deliveries, because unconscious pt is at high risk of pulmonary aspiration of gastric contents. • Indications: • C-Section in certain circumstances. • For shoulder dystocia. • Undiagnosed twins. • Breech presentation.
Rapid sequence induction should be done to prevent aspiration. • Pre-oxygenate mother with 100% O2 as she is prone to hypoxia during intubation 2º to ↓ Functional Residual Capacity & ↑ O2 consumption. • High concentration of Halothane 2% or Isoflurane 3% is used if uterine relaxation is necessary.