Download
1 / 1
10 likes | 108 Views
Paclitaxel and Irinotecan in Platinum Refractory or Resistant Small Cell Lung Cancer: a Galician Lung Cancer Group experience .

E N D
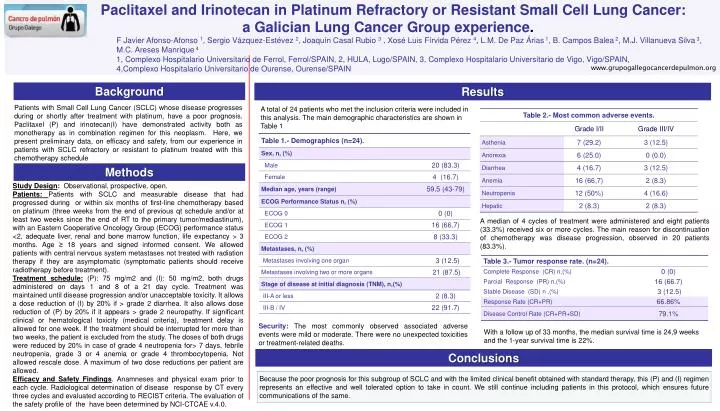
Paclitaxel and Irinotecan in Platinum Refractory or Resistant Small Cell Lung Cancer: • a Galician Lung Cancer Group experience. • F Javier Afonso-Afonso1, Sergio Vázquez-Estévez 2, Joaquín Casal Rubio 3 , Xosé Luis Fírvida Pérez 4, L.M. De Paz Árias 1, B. Campos Balea 2, M.J. Villanueva Silva 3, • M.C. AresesManrique 4 • 1, Complexo Hospitalario Universitario de Ferrol, Ferrol/SPAIN, 2, HULA, Lugo/SPAIN, 3, Complexo Hospitalario Universitario de Vigo, Vigo/SPAIN, • 4,Complexo Hospitalario Universitario de Ourense, Ourense/SPAIN www.grupogallegocancerdepulmon.org Background Results Patients with Small Cell Lung Cancer (SCLC) whose disease progresses during or shortly after treatment with platinum, have a poor prognosis. Paclitaxel (P) and irinotecan(I) have demonstrated activity both as monotherapy as in combination regimen for this neoplasm. Here, we present preliminary data, on efficacy and safety, from our experience in patients with SCLC refractory or resistant to platinum treated with this chemotherapy schedule A total of 24 patients who met the inclusion criteria were included in this analysis. The main demographic characteristics are shown in Table 1 Methods Study Design: Observational, prospective, open. Patients: Patients with SCLC and measurable disease that had progressed during or within six months of first-line chemotherapy based on platinum (three weeks from the end of previous qt schedule and/or at least two weeks since the end of RT to the primary tumor/mediastinum), with an Eastern Cooperative Oncology Group (ECOG) performance status <2, adequate liver, renal and bone marrow function, life expectancy > 3 months.Age ≥ 18 years and signed informed consent. We allowed patients with central nervous system metastases not treated with radiation therapy if they are asymptomatic (symptomatic patients should receive radiotherapy before treatment). Treatment schedule:(P): 75 mg/m2 and (I): 50 mg/m2, both drugs administered on days 1 and 8 of a 21 day cycle. Treatment was maintained until disease progression and/or unacceptable toxicity. It allows a dose reduction of (I) by 20% if > grade 2 diarrhea. It also allows dose reduction of (P) by 20% if it appears > grade 2 neuropathy. If significant clinical or hematological toxicity (medical criteria), treatment delay is allowed for one week. If the treatment should be interrupted for more than two weeks, the patient is excluded from the study. The doses of both drugs were reduced by 20% in case of grade 4 neutropenia for> 7 days, febrile neutropenia, grade 3 or 4 anemia or grade 4 thrombocytopenia. Not allowed rescale dose. A maximum of two dose reductions per patient are allowed. Efficacy and Safety Findings. Anamneses and physical exam prior to each cycle. Radiological determination of disease response by CT every three cycles and evaluated according to RECIST criteria. The evaluation of the safety profile of the have been determined by NCI-CTCAE v.4.0. A median of 4 cycles of treatment were administered and eight patients (33.3%) received six or more cycles. The main reason for discontinuation of chemotherapy was disease progression, observed in 20 patients (83.3%). • Security: The most commonly observed associated adverse events were mild or moderate. There were no unexpected toxicities or treatment-related deaths. With a follow up of 33 months, the median survival time is 24,9 weeks and the 1-year survival time is 22%. Conclusions Because the poor prognosis for this subgroup of SCLC and with the limited clinical benefit obtained with standard therapy, this (P) and (I) regimen represents an effective and well tolerated option to take in count. We still continue including patients in this protocol, which ensures future communications of the same. .






















