Download
1 / 49
490 likes | 610 Views
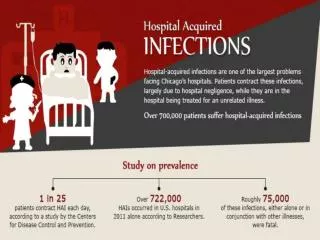
Mandatory Public Reporting of Hospital Infections. Karla Voy, MPH, MS, CIC March 8, 2005. Incidence 1995 1.8 million 4.7 / 100 admissions 9.7 / 1000 pt days 96,000 deaths. Incidence 2004 1.7 million 4.5 / 100 admissions 9.3 / 1000 pt days 99,000 deaths

E N D
Mandatory Public Reporting of Hospital Infections Karla Voy, MPH, MS, CIC March 8, 2005
Incidence 1995 1.8 million 4.7 / 100 admissions 9.7 / 1000 pt days 96,000 deaths Incidence 2004 1.7 million 4.5 / 100 admissions 9.3 / 1000 pt days 99,000 deaths 4.6 million with home and long term care Consensus ConferenceHospital Infections
Consensus Conference • Issue with NNIS benchmarks as a gold standard • Not good enough anymore to be better than the average • 1975 – 2002, IC rate per 1000 pt days up • Inpatient days and ALOS down • Given changes in the population believe we are doing better
Consensus Conference • Trend is down for BSIs • Trend is down for SSIs • SIPP compliance rates • 56% within 1 hour • 41% stopped at 24 hours • 92% appropriate antibiotic selected
Consensus Conference • Antibiotic resistance trends up • Clinician as stakeholder • 95% perceive it as a national problem • 77% as a problem in their institute • 65% in their own practice • Need to put a face in a rate
Consensus Conference • Prevention is primary • Need to bridge evidence-based practice gaps with the reporting of infection rates to determine rate of preventability Denise Cardo, MD, Director, Division of Healthcare Quality Promotion and CDC
Consensus ConferenceThe Consumer • It is a problem – 5-10% of hospitalized patients develop an infection • Costs a lot of money • 90,000 die • Real stories • Secrecy around the situation • Want to give the system a shove
Consensus Conference • No brainer – evidence-based practices • Improve care through awareness and comparative information • HAI is semantics – people do not understand what this is • Public pressure does work Lisa McGiffert, Senior Policy Analyst on Health Issues and the Project Director for StopHospitalInfections.org a project of Consumers Union, publisher of Consumer Reports
Accountability Promote Informed public Market forces deal with poor performers Promotes broader action Learning Promote Clinical judgment leads to better care More useful, credible information Data reflect care Consensus ConferenceHealthcareIndustry
Accountability Guard against Data gamed Data not actionable Improvement agenda hijacked Learning Guard against Actions too slow, small, and diffuse Bad actors still practice Patients kept in the dark Consensus Conference
Consensus Conference • What is needed? • Valid measures • Case finding and data collection specifications • Trusted data collection pathway • Method for verifying data collection • Data analysis methods • Data display options Nancy Foster, VP for Quality and Patient Safety Policy at the American Hospital Association
Consensus ConferenceSurveillance • National Healthcare Safety Network • NNIS (1970-2004) • Nosocomial infections in critical care/surgery pts • NaSH (1999-2004) • Exposure to BBP, TB, Vaccine adverse events • DSN (1996-present) • BSI and vascular access infections dialysis outpts
Consensus Conference • NHSN Components • Patient Safety • Healthcare Personnel Safety • Research and Development • How data are shared in NHSN • A group can enroll in NHSN (i.e., Healthcare organizations, State HDs, Quality Improvement Organizations) • A facility can then join the group and share data
Consensus Conference • Timeline for rollout • 1 – Training and enrollment started in Nov 04; reporting started Jan 05 (NNIS, DSN, NaSH members, special collaborators) • 2 – These members’ “sister” institutions (Mar 05) • 3 – Any healthcare entity (Jul 05) • Internet security still being tested Teresa Horan, MPH, Chief, Performance Measurement Sections at Division of Healthcare Quality Promotion
Consensus Conference • International Perspective • Whatever N. America decides will have a global impact Carthryn Murphy, PhD, Associate Professor, Wollongong University
Consensus ConferenceLiability Issues? • National survey on consumer’s experiences with patient safety and quality information • 34% personal medical error • 21% serious • 16% severe pain • 16% loss of activities • 23% temporary or long term disability • 8% death • 11% initiated malpractice suit
Consensus Conference • Issues with current data • Outdated • No opportunity to show improvement trends • CONFUSING • Different time frames • Different data sources • Different displays • Different scales
Consensus Conference • Potential use by plaintiff’s counsel in an attempt to discredit hospital • Is voluntary reporting of aggregate data enough to constitute waiver from discovery • Confidentiality protections Tammy Lundstrom, MD, VP, Chief Quality and Safety Officer at the Detroit Medical Center
Consensus ConferenceJCAHO – Are we there yet? • Measurement is not a neutral activity – creates stress • Need multiple measures to paint an overall picture • Need risk adjustment • No agreement on whose reporting is better
Consensus Conference • Hospitals with poor surveillance and data collection will look better • No evidence that mandatory reporting is better than voluntary • No one wants to pay for mandatory reporting and it costs • Need built in incentives for voluntary reporting
Consensus Conference • Do not think that legislation in 50 states will fix the problem • Need standardization • Need information technology separate from measuring • Pay for performance – are we robbing peter to pay for paul – leaves hospital without resources when access is already an issue Jerod Loeb, PhD, Executive VP for Research at the JCAHO in Illinois
Consensus Conference21st Century Media • Bogey man with a note pad? • Take press by the hand (wash afterwards) • Counter the problem, offer a solution • What? So What? Now What? • All health care institutions are equal; some more equal than others – public does not differentiate differences • It’s 90 days later; anyone seen the press? (once people understand the differences the issue will become less important) Jim Battaglio, President, Creative Writing Co., Corporate Communications, VP President Emeritus for Hartford Hospital
Consensus Conference • Illinois Perspective • SB 59 - Hospital Report Card Act – effective Jan 2004 • Daily nursing staffing assignments by unit available to public • Quarterly nursing hours per patient, average daily census/hours worked for each clinical service area
Consensus Conference • Mortality • Infections (CDC definitions) • Class I SSI (SIP, then SCIP, hopefully SCIPI) • VAP • CLA-BI • Advisory Group • Begin or end each meeting with a consumer who has a story of infection
Consensus Conference • Develop national standardized measures • Shift to electronic health record now • DOH is developing rules for reporting Patricia Merryweather, Senior VP, Illinois Hospital Association
Consensus Conference • Florida Initiative • HB 1629 – Relating to Affordable Healthcare - passed spring 2004 • Complication rates • Re-admission rates • Infection rates • Not further defined, unfunded • Working group
Consensus Conference • SIP measures • Available/valid/endorsed • Comprehensive Health Information System Advisory Council • Technical workgroup for health care facility web site • Technical workgroup for hospital acquired infections
Consensus Conference • Education of team members is key • Rules published Dec 31, 2004 • Report using CMS criteria and timing • Meeting every 2 weeks • 20-40 people • Rate was initially in rule language, but convinced to move to process measure Loretta Fauerbach, MS, CIC, Director of IC for Shands Hospital at the UF and Shands HealthCare system
Consensus Conference • Missouri SB 1279 - Nosocomial Infection Act of 2004 • Advisory Panel • Consistent with CDC guidelines/standards • MRSA and VRE • Class I SSI • CLA-BI • VAP
Consensus Conference • Reporting rules • Exemptions for hospitals (NNIS approach) • Dec 31, 2005 • Ambulatory surgery clinics (breast, hernia) • June 30, 2005 • CLA-BIs in the ICU • June 30, 2006 • SSIs (hip prosthesis, c-section, CABG)
Consensus Conference • MRSA/VRE – quarterly antibiogram • Whatever hospital is monitoring • Surveillance/colonization cultures excluded • Problems with consumer model legislation • Timing – takes time to do right • Advisory group, outside healthcare – we are the experts • Risk adjustment – no consistent standard Eddie Hedrick, BS, MT (ASCP), CIC, Emerging Infections Coordinator for the Missouri DOH and Senior Services
Consensus Conference • Pennsylvania • Mandated by an independent state agency (PHC4) rather than legislative initiative • Had no opportunity for input – announced Nov 03 with reporting to start in Jan 04 • Challenged and HAI Advisory Panel met Feb 2004 (already collecting data 6 weeks) • Initially PHC4 felt ICP not needed to collect data
Consensus Conference • Urinary catheter UTI • VAP • Catheter-associated BSI • SSI (ortho/musculoskeletal, neurosurgery, circulatory system) • Children’s Hospitals • Inpatient Rehab Facility • Long Term Acute Care Hospitals
Consensus Conference • First data was submitted no later than 6/30/04 • Discrepancy in numbers of infections that hospitals reported to PHC4 for billing purposes and numbers of HAIs reported to PHC4 • Reported to industry/media resulting in bad press
Consensus Conference • PHC4 goal is hospital-wide collection of all HAIs by Jan 1, 2006 • To date, PHC4 has not determined how HAI data will be analyzed/published • Challenge – prevent the preventable
Consensus Conference • Lessons Learned • Focused surveillance ICU loses big picture • Disparity in field on interpretation • UTIs significant cost outside ICU arena • Administration starting to see business case for preventing infections • Can’t keep adding tasks to ICPs without losing value to the process Sharon Krystofiak, MS, MS, MT(ASCP), CIC, Manager of IC at Mercy Hospital in Pittsburgh, PA
Where we stand Feb 5, 2005 • 4 states require mandatory reporting • 32 states with pending legislation
Guidance on Public Reporting of Healthcare-Associated Infections (HICPAC) Feb 28, 2005 • Insufficient evidence on merits/limitations of an HAI public reporting system • Process measures • Target adherence rate (100%) unambiguous • Do not require risk adjustment • Should measure common practice
Guidelines • Process measures • Adherence rates central-line insertion practices • Surgical antimicrobial prophylaxis • Influenza vaccination healthcare personnel/patients/residents
Guidelines • Outcome measures • Frequency, severity, preventability, likelihood they can be detected and reported accurate • Substantial morbidity/mortality/cost • CLA-LCBIs • SSIs
Guidelines • Standardized methods for case-finding • Method to validate • Reporting system can’t produce quality data without adequate resources • Risk adjustment • Reports convey useful/interpretable information to diverse audience
Guidelines • Potential consequences • May reduce HAI rates • May divert resources to reporting infections and collecting data for risk adjustment and away from patient care and prevention
Guideline Recommendations • Use established public health surveillance methods when designing and implementing mandatory HAI reporting systems • Create a multidisciplinary advisory panel to monitor the planning and oversight of the operations and products of HAI public reporting systems
Recommendations • Choose appropriate process and outcome measures based on facility type and phase in measures gradually to allow time for facilities to adapt and to permit ongoing evaluation of data validity • Provide regular and confidential feedback of performance data to healthcare providers
Ohio HB 541 • Met with Rep Raussen • Letter delivered with one voice from all Ohio APIC Chapters • Establish Advisory Group • Chartered with specific responsibilities • Phased approach/Florida as example
HB 541 • Proposed Performance outcome data • Number of cases • Average billed charge • Average LOS • Readmission rate • Complication rate • Mortality rate • Infection rate - % of pts develop an infection while admitted to hospital • Whether electronic system used to order drugs
HB 541 • Maintaining communication with his office • Awaiting final version of bill (number will change) • Spokespersons selected to represent/maintain communication/answer questions for Rep Raussen’s office
Key Stakeholders/Special Interest Groups • Consumers Union • http://www.sonsumersunion.org/campaigns/stophospitalinfections/learn.html • Committee to REDUCE INFECTION RATES (RID) • http://www.hospitalinfectionrates.org/ • The Leapfrog Group • http://www.leapfrogfroup.org • Services Employee International Union (SEIU) • http://www.seiu.org/health/nurses/safe_staffing/fed_leg_studies.cfm