Download
1 / 18
180 likes | 373 Views
Thyroid & neurological disorders in pregnancy. Dr.Roaa H. Gadeer MD. Physiology of thyroid function. TSH is released from anterior pituitary in 1-2 hrs cycle → thyroxin (T4) & triiodothyronin (T3).

E N D
Thyroid & neurological disorders in pregnancy Dr.Roaa H. Gadeer MD
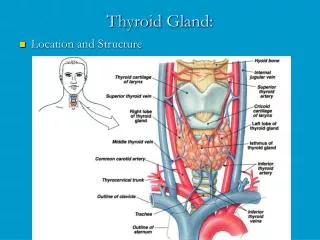
Physiology of thyroid function • TSH is released from anterior pituitary in 1-2 hrs cycle → thyroxin (T4) & triiodothyronin (T3). • 75% of T4 & T3 are bound to thyroid-binding globulin (TBG), the rest bound to albumin and transthyretin. • Free T4=0.04% and free T3=0.05%. • Iodine is trapped by the gland and converted to iodide to synthesize thyroglobulin. Each molecule carries 3-4 molecules of T4. • T3 is produced by peripheral deiodination of T4 and it is 3 times more potent than T4.
Physiology of thyroid function • In pregnancy: - TBG ↑ in first 2 wks to reach a plateau at 20 wks due to ↑ Oestrogen level . - ↑ TBG → ↑ serum T4 & T3 with no change in free T4 & T3. • Iodine deficiency (↑GFR + fetal thyroid uptake) → ↑ thyroid gland uptake & enlargement (goitre). • hCG occupies TSH receptors → ↓TSH but it stimulates the gland → ↑ T4. • Placental conversion of T4 to T3 to prevent excess T4 & even low T4 level in late pregnancy.
Fetal thyroid function • Firsttrimester: fetus needs maternal T4 for brain development. • Small amount of maternal T4 crosses placenta before 12 wks. • Maternal T3,T4 & TSH does not cross the placenta after 12 wks. • Fetal thyroid produces T3 & T4 after 10 wk’s gestation & reaches the adult levels at 36 wks. • Thyrotropin-releasing hormone (TRH) & iodine cross the placenta
Aetiology & management • Iodine deficiency: - maternal gland has a greater affinity to iodide than placenta and fetus resulting in cretinism. • Fetal neocortex and basal ganglia are sensitive to iodine deficiency resulting in mental retardation. • Management: • Preconceptional iodine and up to second trimester. • Iodination of water, salt or flour
Hyperthyroidism • Occurs in approximately 1 in 500 pregnancies. • In pregnancy it is due to Grave’s disease (90% to 95%).. • Graves' disease is an autoimmune disease results in production of thyroid-stimulating antibody (TSA), which mimics TSH and stimulates thyroid function and size increase. • Less common causes: toxic adenoma, toxic multinodular goiter, subacute thyroiditis, TSH producing pituitary tumor, metastatic follicular cell carcinoma, and painless lymphocytic thyroiditis. • Pregnancy-related causes: hyperemesis gravidarum, gestational trophoblastic disease (GTD), and struma ovarii
Hyperthyroidism • signs and symptoms: tachycardia > 100 bpm, exophthalmos, thyromegaly, onycholysis (reflect the disease activity), and poor weight gain with good appetite. • Symptoms: fatigue and heat intolerance not useful (common in pregnancy). • laboratory test results: increase in serum T4 level and increase in the FT4 index • Complications: pre-eclampsia, thyroid storm, or CHF for the mother, and preterm labour and delivery, IUGR, and stillbirth
HyperthyroidismTreatment • Is similar to non-pregnant women. • Radioactive iodine is containdicated. • Drugs: • propylthiouracil (PTU) or carbimazole and beta-blockers. • use the minimum dose as they cross the placenta causeing fetal hypothyroidism and goiter. • Both not teratogenic. Not contraindicate breastfeeding. • Both reduce TSH receptors antibodies titer → inhibition of T4 production. • PTU inhibits incorporation of iodine into tyrocine and peripheral conversion of T4 toT3.
Hypothyroidism • hypothyroidism is uncommon (1%), because it is associated with infertility. • Causes: autoimmune Hashimoto’s thyroiditis (usaully), idiopathic myoedema, treatment of hyperthyroidism, type 1 diabetes is associated with an increased incidence of subclinical hypothyroidism during pregnancy. • Signs and Symptoms: Asymptomatic, weight gain, lethargy, weakness, cold sensitivity, hair loss, myxedematous changes, and dry skin. TSH level is increased; serum T4 level is low; and the FT4 index is decreased.
Hypothyroidism • Treatment: • L-thyroxin, starting at 0.05 to 0.10 mg daily. • The dosage should be increased over several weeks the goal is normal laboratory values and resolve of the patient's symptoms. • A maximum dosage of 0.2 mg/d of L-thyroxin should not be exceeded . • TSH level alone can be followed to determine optimal dosing. • Complications: pre-eclampsia, IUGR, abruptio placentae, anaemia, postpartum haemorrhage, stillbirth, and cardiac dysfunction. • Fetal thyroid: not affected..
Nodular thyroid disease • Evaluation: Ultrasound, and fine-needle aspiration or tissue biopsy • If thyroid carcinoma is found, surgical excision is the primary treatment and should not be postponed because of pregnancy
Epilepsy • Incidence: 6/1000 pregnancy. • Seizure frequency may increase, decrease or no change (37%, 13% and 50% respectively). • Fetal anomalies ↑ in epileptic mother. • Anti-epileptic drugs (AED) responsible of most of fetal anomalies. • Control of seizures outweigh the risks • Polytherapy with (AED) caries more risks than monotherapy. • High doses of folic acid reduces fetal anomalies. • Lower doses of AED carry lower risk of fetal anomalies. • Patients not taking drugs or having regular seizures carry ↑ risk.
Causes of epilepsy • Idiopathic epilepsy. • Intracranial infections: meningitis/encephalitis/brain abscess… • Vascular disease :cerebral infarction/eclampsia/sub-arachnoid haemorrhage. • Metabolic: liver & renal failure/hponat.glyc.calceamia….. • Drug toxicity: tricyclic antidepressant/local anesthesia (lignocain) • Secondary to specific cause: trauma/intracranial mass/Aps…
Drugs used in epilepsy • Enzyme-inducing AED: • Phenobarbitone • Phenytoin. • carbamazepine • Non-enzyme-inducing AED: • valproate. • Gabapentin. • Lamotrigine. • clonazepam
Management of epilepsy • Pre-pregnancy counseling: • Stop AED in patients having no seizure for 2 years. • Use single AED with low dose. • Folic acid 5 mg/day (sp. Carbamazepine & valproate). • Antenatal management: • Screening for fetal anomalies. • Oral vitamin K 10 mg/day from 36 wks onwards to prevent hemorrhage. • Women adviced to take shower rather than bath. • If storoid is given for obstetric indication it should be within 48 hrs (24 mg dexamethazone 24 hrs apart)
Management of epilepsy • Intrapartum care: • Vaginal delivery is advised. • Seizures ↑: sleep disturbance, ↓ drug intake and absorption & hyperventilation (make sure that the drugs has been took). • Seizures during labour are best controlled with IV benzodiazepines (diazepam/clonazepam) • Postpartum care: • Encourage breastfeeding (rare neonatal effects). • A single 1 mg of vitamin K to the neonate is advisable. • Contraception: enzyme-inducing AED reduce the efficacy so 50 ug oestrogen, reduce the free interval to 5-6 days, depo-provera is used every 10 wks & mirena is ideal (progesterone not affected enzyme-inducing AED ).