Download
1 / 16

E N D
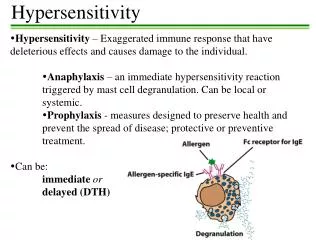
1. Good afternoon, ladies and gentlemen.
I am Dr.Priti Bajaj from Aalborg Hospital and University, Denmark and am working as a research fellow in the department of Obstetrics and Gynecology.
The aim of my talk today is to present to you briefly the somatosensory changes at referral areas of menstrual pain in healthy women, in order to speculate the mechanisms responsible for the phenomenon of referred pain related to the female reproductive organs.Good afternoon, ladies and gentlemen.
I am Dr.Priti Bajaj from Aalborg Hospital and University, Denmark and am working as a research fellow in the department of Obstetrics and Gynecology.
The aim of my talk today is to present to you briefly the somatosensory changes at referral areas of menstrual pain in healthy women, in order to speculate the mechanisms responsible for the phenomenon of referred pain related to the female reproductive organs.
2. Health surveys in both America and Europe show that 40% of women's overall morbidity and use of health care is predominantly related to gynecological and obstetrical problems, with Menstrual pain and pelvic pain accounting for the most common complaints during the reproductive period . Inspite of this, the currently available empirical pain treatment strategies employed are often not successful for patients with gynecologic pain. Health surveys in both America and Europe show that 40% of women's overall morbidity and use of health care is predominantly related to gynecological and obstetrical problems, with Menstrual pain and pelvic pain accounting for the most common complaints during the reproductive period . Inspite of this, the currently available empirical pain treatment strategies employed are often not successful for patients with gynecologic pain.
3. Pain research associated with the reproductive organs has been conducted mainly in animals and suggests that differences in nociception related to the reproductive cycle maybe due to hormonal influences. Repetition of animal studies in humans is required to develop more meaningful treatment strategies.
Majority of human pain research has mainly related to somatic tissues, but these results cannot be completely applied to the visceral domain due to differences between visceral and somatic pain.
An interesting association is that of gastrointestinal symptoms with menstruation. One-third of otherwise asymptomatic women experience gastrointestinal symptoms that vary across the menstrual cycle. Understanding the physiological variations and the relationship with pelvic pain are important as they could be related to ovarian hormone levels which vary with the menstrual cycle.
Pain research associated with the reproductive organs has been conducted mainly in animals and suggests that differences in nociception related to the reproductive cycle maybe due to hormonal influences. Repetition of animal studies in humans is required to develop more meaningful treatment strategies.
Majority of human pain research has mainly related to somatic tissues, but these results cannot be completely applied to the visceral domain due to differences between visceral and somatic pain.
An interesting association is that of gastrointestinal symptoms with menstruation. One-third of otherwise asymptomatic women experience gastrointestinal symptoms that vary across the menstrual cycle. Understanding the physiological variations and the relationship with pelvic pain are important as they could be related to ovarian hormone levels which vary with the menstrual cycle.
4. The referral area of visceral pain are segmental and are to muscles and skin innervated by the same spinal nerves that innervate the viscus giving rise to the referred sensation.
Information regarding sensitivity changes across the menstrual cycle in the referral pain areas may increase our knowledge of viscerosomatic convergence mechanisms and the mechanisms involved in the generation and maintenance of pain from the female reproductive organs. Sensitivity changes at referral pain areas can be demonstrated by the phenomenon of hyperalgesia which is a decrease in the PT or an increased sensitivity to painful stimuli
Referral areas of pain from the uterus are mainly related to the thoracic T10-T12 segments and sacral S2-S4 segments , as shown in the figure. For our study we selected as referral areas two sites located symmetrically on the right and left abdomen, lateral to the navel and one site in the midline of the lower back.
The lateral surface of the upper arm and anterior surface of the mid-thigh were the Non-referral control areas. The referral area of visceral pain are segmental and are to muscles and skin innervated by the same spinal nerves that innervate the viscus giving rise to the referred sensation.
Information regarding sensitivity changes across the menstrual cycle in the referral pain areas may increase our knowledge of viscerosomatic convergence mechanisms and the mechanisms involved in the generation and maintenance of pain from the female reproductive organs. Sensitivity changes at referral pain areas can be demonstrated by the phenomenon of hyperalgesia which is a decrease in the PT or an increased sensitivity to painful stimuli
Referral areas of pain from the uterus are mainly related to the thoracic T10-T12 segments and sacral S2-S4 segments , as shown in the figure. For our study we selected as referral areas two sites located symmetrically on the right and left abdomen, lateral to the navel and one site in the midline of the lower back.
The lateral surface of the upper arm and anterior surface of the mid-thigh were the Non-referral control areas.
5. Human studies have shown hyperalgesia at referred pain areas of renal / ureteric / biliary calculosis and in experimentally induced gastrointestinal and bladder pain. In addition, temporal summation effect of pain has been shown by repeated stimulation of the gastrointestinal tract and urinary bladder.
However, few studies have focused on referred areas related to gynecological pain and inconsistent effects have been demonstrated in the pattern of changes in pain sensitivity in women across the menstrual cycle . It is not known whether repetitive uterine stimulation resulting from menstruation is able to generate referred nociception and somatosensory changes at referred areas.
�Temporal summation is the phenomenon where a single nociceptive stimulus by repetition causes exaggerated pain responses in humans.� It has been demonstrated by electrical stimulation of the gastrointestinal tract and distension of the urinary bladder, leading to increased pain perception.
In the course of every menstrual cycle, the uterus is exposed repeatedly to chemical stimulation (prostaglandins, vasopressin and leukotrines), ischemia and mechanical stimulation in the form of increased uterine contractions Human studies have shown hyperalgesia at referred pain areas of renal / ureteric / biliary calculosis and in experimentally induced gastrointestinal and bladder pain. In addition, temporal summation effect of pain has been shown by repeated stimulation of the gastrointestinal tract and urinary bladder.
However, few studies have focused on referred areas related to gynecological pain and inconsistent effects have been demonstrated in the pattern of changes in pain sensitivity in women across the menstrual cycle . It is not known whether repetitive uterine stimulation resulting from menstruation is able to generate referred nociception and somatosensory changes at referred areas.
�Temporal summation is the phenomenon where a single nociceptive stimulus by repetition causes exaggerated pain responses in humans.� It has been demonstrated by electrical stimulation of the gastrointestinal tract and distension of the urinary bladder, leading to increased pain perception.
In the course of every menstrual cycle, the uterus is exposed repeatedly to chemical stimulation (prostaglandins, vasopressin and leukotrines), ischemia and mechanical stimulation in the form of increased uterine contractions
6. Thus, the aims of the present study were to evaluate if cyclic nociceptive visceral activation, resulting from menstruation is capable of generating referred somatosensory changes in response to various pain stimulation modalities. In addition, variations in somatosensory changes at the different body sites were compared in females and males.
The hypothesis for the present study were that psychophysical responses to different nociceptive stimuli vary across the menstrual cycle and repetitive nociceptive visceral activation, resulting from menstruation would be capable of generating referred somatosensory changes.
Thus, the aims of the present study were to evaluate if cyclic nociceptive visceral activation, resulting from menstruation is capable of generating referred somatosensory changes in response to various pain stimulation modalities. In addition, variations in somatosensory changes at the different body sites were compared in females and males.
The hypothesis for the present study were that psychophysical responses to different nociceptive stimuli vary across the menstrual cycle and repetitive nociceptive visceral activation, resulting from menstruation would be capable of generating referred somatosensory changes.
7. In order to study the somatosensory changes, we assessed the pain threshold at the referred and non.referred areas of menstrual pain. The pain stimulation modalities used are illustrated in the figure. The contact heat thermode was used for assessing the heat pain threshold, the pressure algometer for assessing the pressure and pinch pain threshold and the von Frey fibres to assess the pinprick threshold.In order to study the somatosensory changes, we assessed the pain threshold at the referred and non.referred areas of menstrual pain. The pain stimulation modalities used are illustrated in the figure. The contact heat thermode was used for assessing the heat pain threshold, the pressure algometer for assessing the pressure and pinch pain threshold and the von Frey fibres to assess the pinprick threshold.
8. 15 female students , aged 22 - 38 years, with regular menstrual cycles ranging from 28-34 days, who were not on oral contraceptives and had no history of dysmenorrhea participated in the study.
10 male students aged 24 - 36 years were the controls.
15 female students , aged 22 - 38 years, with regular menstrual cycles ranging from 28-34 days, who were not on oral contraceptives and had no history of dysmenorrhea participated in the study.
10 male students aged 24 - 36 years were the controls.
9. Experiment sessions were repeated four times during one menstrual cycle , which was divided into 4 phases as shown. At each experimental session the pinch, pressure, heat and pinprick pain threshold (PT) were assessed at the five sites. The sequence of initial menstrual phase investigated, sites tested and stimulation modality used were randomised to minimise order effects.
Experiment sessions were repeated four times during one menstrual cycle , which was divided into 4 phases as shown. At each experimental session the pinch, pressure, heat and pinprick pain threshold (PT) were assessed at the five sites. The sequence of initial menstrual phase investigated, sites tested and stimulation modality used were randomised to minimise order effects.
10. The descriptive statistics are reported as mean ? SEM. A two-way repeated measures analysis of variance (ANOVA) was performed to compare differences and interactions between the pain thresholds, areas examined and the menstrual cycle phases.
In females, Significantly lower pain thresholds were detected in the ovulatory phase as compared to the other menstrual phases for heat stimulation at the abdomen . Significantly lower heat PT were evident at the abdominal and back referral areas as compared to the non-referral areas in all phases of the menstrual cycle. In males however, no significant differences in the heat PT were detected between referral and non-referral areas .
The descriptive statistics are reported as mean ? SEM. A two-way repeated measures analysis of variance (ANOVA) was performed to compare differences and interactions between the pain thresholds, areas examined and the menstrual cycle phases.
In females, Significantly lower pain thresholds were detected in the ovulatory phase as compared to the other menstrual phases for heat stimulation at the abdomen . Significantly lower heat PT were evident at the abdominal and back referral areas as compared to the non-referral areas in all phases of the menstrual cycle. In males however, no significant differences in the heat PT were detected between referral and non-referral areas .
11. In females, significantly lower pressure pain thresholds were detected in the ovulatory phase as compared to the other menstrual phases for pressure stimulation at the back .
Significantly lower pressure PT were evident at the abdominal referral areas as compared to the non-referral areas in all phases of the menstrual cycle. In males no significant differences in the pressure PT were detected between referral and non-referral areas .
In females, significantly lower pressure pain thresholds were detected in the ovulatory phase as compared to the other menstrual phases for pressure stimulation at the back .
Significantly lower pressure PT were evident at the abdominal referral areas as compared to the non-referral areas in all phases of the menstrual cycle. In males no significant differences in the pressure PT were detected between referral and non-referral areas .
12. The pinch PT at the abdominal and back referral areas did not vary in the different menstrual phases.
The pinch PT at the back was significantly greater than at the abdomen and non-referral areas in both males and females.The pinch PT at the abdominal and back referral areas did not vary in the different menstrual phases.
The pinch PT at the back was significantly greater than at the abdomen and non-referral areas in both males and females.
13. There were no significant differences in the pinprick threshold between referral and non-referral areas in females or males.
There were no significant differences in the pinprick threshold between referral and non-referral areas in females or males.
14. To summarise the results, we have demonstrated modality specific hyperalgesia in females to heat and pressure stimulation at referral areas of menstrual pain across all phases of the menstrual cycle with significantly increased sensitivity in the ovulatory phase, as compared to the other phases of the menstrual cycle.
Males did not demonstrate the same pattern of hyperalgesia as females for heat and pressure stimulation.
To summarise the results, we have demonstrated modality specific hyperalgesia in females to heat and pressure stimulation at referral areas of menstrual pain across all phases of the menstrual cycle with significantly increased sensitivity in the ovulatory phase, as compared to the other phases of the menstrual cycle.
Males did not demonstrate the same pattern of hyperalgesia as females for heat and pressure stimulation.
15. Conclusions Increased pain sensitivity demonstrated in the ovulatory phase suggests that LH and oestrogen levels may modulate tenderness, and possibly pain perception in women.
Central sensitisation subsequent to repeated nociceptive uterine stimulation is likely to be the neurophysiologic substrate of hyperalgesia at referral areas of menstrual pain across all phases of the menstrual cycle. We conclude from these results that increased pain sensitivity demonstrated in the ovulatory phase suggests that LH and oestrogen levels may modulate tenderness, and possibly pain perception in women.
Central sensitisation subsequent to repeated nociceptive uterine stimulation is likely to be the neurophysiologic substrate of hyperalgesia at referral areas of menstrual pain across all phases of the menstrual cycle.
We conclude from these results that increased pain sensitivity demonstrated in the ovulatory phase suggests that LH and oestrogen levels may modulate tenderness, and possibly pain perception in women.
Central sensitisation subsequent to repeated nociceptive uterine stimulation is likely to be the neurophysiologic substrate of hyperalgesia at referral areas of menstrual pain across all phases of the menstrual cycle.
16. Additional research related to the development of modality-specific hyperalgesia at referral areas of menstrual pain is needed to further extend this work.
I would like to thank my supervisors Prof Lars Arendt Nielsen and Professor Hans Madsen, and my husband Dr.Prem Bajaj for advising and guiding me at all phases of this study . I would also like to thank the technical & administrative staff for all the help rendered and ofcourse all the subjects whose participation made this study possible.Additional research related to the development of modality-specific hyperalgesia at referral areas of menstrual pain is needed to further extend this work.
I would like to thank my supervisors Prof Lars Arendt Nielsen and Professor Hans Madsen, and my husband Dr.Prem Bajaj for advising and guiding me at all phases of this study . I would also like to thank the technical & administrative staff for all the help rendered and ofcourse all the subjects whose participation made this study possible.