Download
1 / 42
430 likes | 559 Views
Pharmacological management Blood glucose-lowering medicines. Aims of treatment. Reduce the symptoms of hyperglycaemia Limit adverse effects of treatment Maintain quality of life and psychological well-being Prevent or delay vascular complications of diabetes. 0. 3. 6. 9. 12. 15.

E N D
Pharmacological managementBlood glucose-lowering medicines Slides current until 2008
Aims of treatment • Reduce the symptoms of hyperglycaemia • Limit adverse effects of treatment • Maintain quality of life and psychological well-being • Prevent or delay vascular complications of diabetes Slides current until 2008
0 3 6 9 12 15 UKPDS:long-term glucose control 9 Conventional 8 HbA1c (%) Intensive 7 6 0 Years of treatment UKPDS Study Group 1998 Slides current until 2008
Natural history of type 2 diabetes Henry 1998 Slides current until 2008
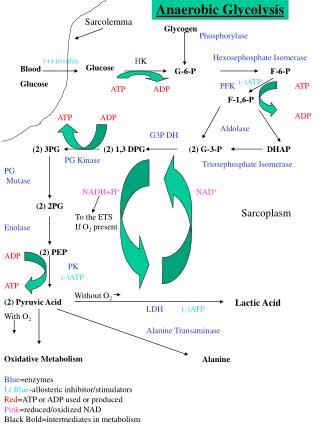
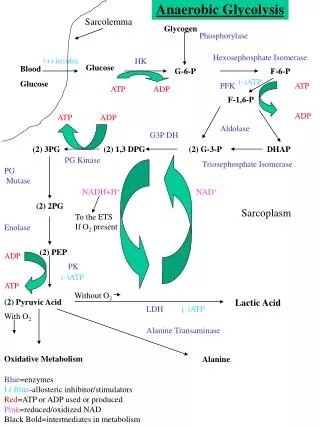
Mechanisms of action GLP-1 (incretins) improve response to glucose level Biguanides and thiazolidinediones reduce glucose production Insulin secretagogues: sulphonylureas and meglitinides increase insulin production Alpha-glucosidase inhibitors slow absorption of sucrose and starch Thiazolidinediones and biguanides reduce insulin resistance Slides current until 2008
Understanding the names • Chemical name relates to chemical structure • Generic name identifies a unique compound with therapeutic properties • Brand name given by the manufacturer Slides current until 2008
What are the most common oral blood glucose-lowering medicines in your community? • What are their brand names and generic names? Slides current until 2008
The principles of combination therapy • Two (or more) oral blood glucose-lowering medicines that have different mechanisms of action • Two medications rather than increase in initial medicine to maximum dosage • Fewer side effects than mono-therapy at higher doses Slides current until 2008
Expected effect of blood glucose-lowering medicines Canadian Diabetes Association 2003 Slides current until 2008
Strategies to help people remember • Check that people understand how and when to take their medicines • Clarify the benefits of treatment • Keep regimens simple • Minimize costs • Discuss adverse effects Rubin 2005 Slides current until 2008
Targets for blood glucose 1CDA 2003, 2ADA 2004, 3 IDF 2005 Slides current until 2008
Suggested starting medicine CDA 2003 Slides current until 2008
Increasing or adding • If goals have not been reached within 2-3 months, medication should be increased or medication from a different class added • Target levels should be reached within 6 months • Insulin should be added if necessary to reach target levels Slides current until 2008
Biguanides • Action not fully understood • Decreases glucose production in liver • Mild and variable effect on muscle sensitivity to insulin Side effects • Gastrointestinal (nausea, abdominal discomfort or diarrhea and occasional constipation) • Lactic acidosis Slides current until 2008
Biguanides Contraindications • Renal insufficiency • Liver failure • Heart failure • Severe gastrointestinal disease Advantages • Do not cause hypoglycaemia when used as mono-therapy • Do not cause weight gain; may contribute to weight loss Slides current until 2008
Biguanides First-line treatment in overweight or obese people • Do not cause weight gain • Have some effect on resistance at the periphery Slides current until 2008
Biguanides Caution • Should be discontinued 24 hours before procedures requiring intravenous contrast dye • Can be restarted 48 hours after the procedure if renal function is not compromised Slides current until 2008
Sulphonylureas • Increase insulin secretion regardless of blood glucose levels • Many different medicines in this class Side effects • Hypoglycaemia • Stimulate appetite and provoke weight gain • Nausea, fullness, heartburn • Occasional rash • Swelling Slides current until 2008
Sulphonylureas Short-acting secretagogues Meglitinides – increase insulin secretion in response to increasing blood glucose levels (i.e. after eating) Side effects • Hypoglycaemia (probably less than sulphonylureas) • Weight gain Slides current until 2008
Sulphonylureas Contraindications • Type 1 diabetes • Pregnancy • Breastfeeding Sulphonylureas - Use cautiously with liver or kidney disease Meglitinides - Severe impairment of liver function Slides current until 2008
Sulphonylureas Things to remember • Some sulphonylureas have slower onset and lower peak than glyburide, thus may provoke less hypoglycaemia • Some need to be taken only once a day, therefore may be easier to remember to take • First generation sulphonylureas, such as chlorpropamide may accumulate and cause hypoglycaemia due to their long duration of action Slides current until 2008
Thiazolidinediones • Improve sensitivity to insulin in muscle, adipose tissue and liver • Reduce glucose output from liver • Changes fat distribution by decreasing visceral fat and increasing peripheral fat Side effects • Weight gain, fluid retention • Upper respiratory infection and headache • Decrease in haemoglobin Slides current until 2008
Thiazolidinediones Contraindications • Liver disease, heart failure or history of heart disease • Pregnancy and breast feeding They are not contraindicated in renal insufficiency Potential benefits • Reduced levels of LDL-cholesterol and increased level of HDL-cholesterol Slides current until 2008
Alpha glucosidase inhibitors • Slow digestion of sucrose and starch and therefore delay absorption • Slow post-meal rise in blood glucose Side effects • Flatulence, abdominal discomfort , diarrhoea • As mono-therapy will not cause hypoglycaemia • Hypoglycaemia when used with other medicine (e.g. a sulphonylurea) Slides current until 2008
Alpha glucosidase inhibitors Contraindications • Intestinal diseases, such as Crohn’s • Autonomic neuropathy affecting the gastro-intestinal tract Must be taken just before a meal Slides current until 2008
GLP-1 (incretin mimetic agent) • Improves beta-cell responsiveness to increasing glucose levels • Decreases glucagon secretion • Slows gastric emptying • Results in a feeling of fullness • Must be injected subcutaneously twice a day, within 30-60 minutes before a meal • Reduces HbA1c by ~1% Side effects • Nausea • Weight loss • Diarrhoea • Risk of hypoglycaemia when used with a sulphonylurea Slides current until 2008
GLP-1 (incretin mimetic agent) Contraindications • End-stage kidney disease or renal impairment • Pregnancy • Severe gastrointestinal disease Slides current until 2008
DPP-4 InhibitorsA new class of medications called DPP-4 inhibitors help improve A1C without causing hypoglycemia. They work by by preventing the breakdown of a naturally occuring compound in the body, GLP-1. GLP-1 reduces blood glucose levels in the body, but is broken down very quickly so it does not work well when injected as a drug itself. By interfering in the process that breaks down GLP-1, DPP-4 inhibitors allow it to remain active in the body longer, lowering blood glucose levels only when they are elevated. DPP-4 inhibitors do not tend to cause weight gain and tend to have a neutral or positive effect on cholesterol levels. Sitagliptin(Januvia), saxagliptin(Onglyza) and Vidagliptin(Galvus) are currently DPP-4 inhibitors on the market .ADA Slides current until 2008
Older people with diabetes Beware of the possible reductions in • General good health (with other concomitant conditions) • Kidney function (and increased risk of hypoglycaemia) • Family support and monitoring • Vision • Flexibility and activities of daily living Remember also • Poly-pharmacy increases the risk of medicine-related adverse events • To review all medication and complementary therapies Slides current until 2008
Older people with diabetes • Always start with the lowest dose of any blood glucose-lowering medicine and increase gradually • Using shorter-acting medicines reduces the risk of hypoglycaemia • Hypoglycaemia may increase the risk of falls and heart attack in older people Slides current until 2008
Older people with diabetes Remember the possibility of • Forgetfulness • Poor motivation • Depression • Cognitive deficits • Poly-pharmacy • Reduced manual dexterity These impact on the ability to maintain self-care and achieve maximum benefits from blood glucose-lowering medicines. Slides current until 2008
Ineffectiveness of blood glucose-lowering medicines If oral blood glucose-lowering medicines are ineffective • Check diet and exercise • Consider adding intermediate or long-acting insulin at bedtime • Maintain metformin • Consider reducing or stopping the morning sulphonylurea Slides current until 2008
Case study • AB has had type 2 diabetes for two years • 51-year-old truck driver • BMI of 32, blood pressure at 150/95 • HbA1C 9.5% • No medication • AB says he has no time for exercise and will not change his meal pattern What medication do you think should be started and why? Slides current until 2008
Summary • Lifestyle changes first • Start medicine as soon as needed • Add a different kind • No delay starting insulin Slides current until 2008
Review question 1. Which of the following adverse reactions are most likely due to metformin therapy? • Oedema • Diarrhea • Heart failure • Weight gain Slides current until 2008
Review question 2. Which of the following statements best describes alpha-glucosidase inhibitors? • Likely to cause weight gain • Should be taken with first bite of the meal • Commonly associated with hypoglycaemia • Well tolerated, few side effects Slides current until 2008
Review question 3. Which statement is FALSE? • All oral medicines used to treat diabetes should be discontinued once insulin is started • In most people, blood glucose-lowering medicines become less effective over time • Blood glucose-lowering medicines from different classes are often used in combination to reach target blood glucose • It is important to be physically active and follow a prescribed meal plan in addition to blood glucose-lowering medicines Slides current until 2008
Review question JL is a 45-year-old man. He has been taking 5 mg glyburide and 500 mg metformin at breakfast and supper. His fasting blood glucose ranges from 5.3–6.7mmol/L but he has been experiencing hypoglycaemia most days at 3 or 4 pm. 4. What is the likely cause of JL’s low blood sugars? • Breakfast metformin • Supper metformin • Breakfast glyburide • Supper glyburide Slides current until 2008
Review question 5. When filling his prescription for a sulphonylurea, what is the most important thing to discuss with John? • What and when to eat • When to take the medication • How to recognize and treat hypoglycaemia • When to see his doctor again Slides current until 2008
Answers • b • b • a • c • c Slides current until 2008
References • UK Prospective Diabetes Study (UKPDS) Group. Intensive blood glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in person with diabetes with type 2 diabetes (UKPDS 33). Lancet 1998; 352: 837-53. • Ahmann AJ, Riddle MC. Current blood glucose lowering medicines for type 2 diabetes. Postgrad Med 2002; 111(5): 32-46. • Henry RR. Type 2 diabetes care: the role of insulin-sensitizing agents and practical implications for cardiovascular disease prevention. Am J Med 1998; 105(1A): 20S-26S. • Luna B, Feinglos MN. Blood glucose-lowering medicines in the management of type 2 diabetes mellitus. Am Fam Physician2001; 63(9): 1747-56. • Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Can J Diab 2003; 27(supple 2). • Yki-Jarvinnen H, Ryysy L, Nikkila K, et al. Comparison of bedtime insulin regimen in person with diabetes with type 2 diabetes mellitus; a randomized control trial. Annals Intern Med1999; 130(5): 89-96. • Amylin Pharmaceuticals Inc and Eli Lilly & Co. Byetta (cited 2005July 25) (16 screens). (Available from: http://www.byetta.com) • Rubin Rr. Adherence to pharmacologic therapy in patients with type 2 diabetes mellitus. Am J Med 2005; 118(5A): 275-345. Slides current until 2008