Download
1 / 30
310 likes | 387 Views
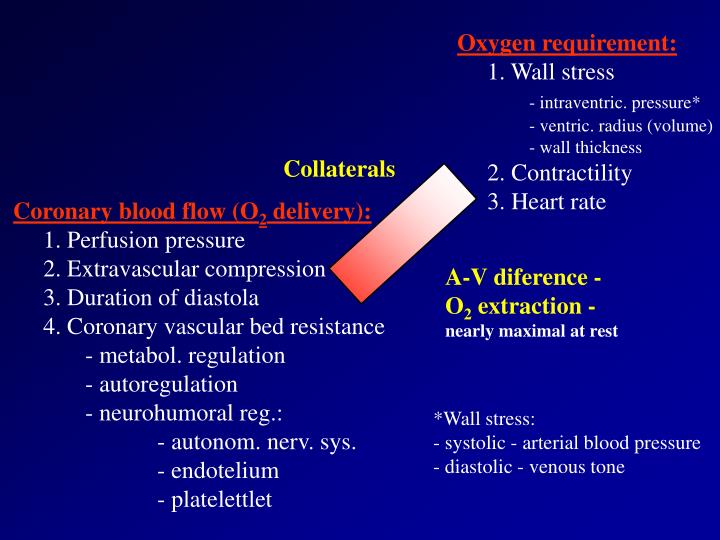
Oxygen requirement: 1. Wall stress - intraventric. pressure* - ventric. radius (volume) - wall thickness 2. Contractility 3. Heart rate. Collaterals. Coronary blood flow (O 2 delivery): 1. Perfusion pressure 2. Extravascular compression 3. Duration of diastola

E N D
Oxygen requirement: 1. Wall stress - intraventric. pressure* - ventric. radius (volume) - wall thickness 2. Contractility 3. Heart rate Collaterals Coronary blood flow (O2 delivery): 1. Perfusion pressure 2. Extravascular compression 3. Duration of diastola 4. Coronary vascular bed resistance - metabol. regulation - autoregulation - neurohumoral reg.: - autonom. nerv. sys. - endotelium - platelettlet A-V diference - O2 extraction - nearly maximal at rest *Wall stress: - systolic - arterial blood pressure - diastolic - venous tone
Angina Pectoris - primary cause is an inbalance between the oxygen requirement of the heart and the oxygen supplies to it via the coronary vessels. - absolute - obstruction of the coronary vessels - relative - increase in oxygen requirement, coronary arteries are without obstruction
Etiology Disease perfusion of myocardium Disease oxygen reqiurement Atherosclerosis Stenosis or insuf. of aortal valve Angiospasm Systemic hypertension Systemic artery disese Hypertrophic cardiomyopathy Pulmonary hypertension - diabetic microangiopathy Other dis. of coronary arteries - congenital defects - A-V anastomosis - traumatic changes - embolism
PATHOPHYSIOLOGY - mechanism Atheromatous plaque - excentric - concentric Trombosis Spasm
Acute (unstable) angina unstable angina acute myocardial infarction sudden death Chronic (stable) angina Angina of effort Vasospastic angina Silent ischemia IHD manifested by heart failure IHD manifested by arrhythmias
Principles of therapy of Angina: improvement quality of live ( symptoms/pain episodes). improvement of prognosis Design: Therapy of atherosclerosis. perfusion of impaired area. Prevention of trombotic occlusion. Therapy of risk factors
ORGANIC NITRATES are used for relief of anginal pain, and in unstable angina. 1. "acute" prophylaxis - Glyceryl trinitrate(TNT) - generally best used as - sublingually (0.3 - 0.5 mg tabl., 0.4 mg spray) - i.v. infusion (5-200 mg/min). 2. "longer" prophylaxis - TNT - transdermally, SR tablets Alternatively, a longer acting nitrate such as isosorbide mononitrate or isosorbide dinitrate (which is converted to the mononitrate in the body) may be used. Isosorbide mononitrate is less expensive than GTN patches and is taken by mouth.
Mechanism of action Glyceryl trinitrate works by relaxing vascular smooth muscle. It is metabolized by glutathione S-transferase in the smooth muscle cells with generation ofnitric oxide (NO). Release of NO from TNT apparently requires sulfydryl groups from a stereospecific intermediary. Exhaustion of this sulfydryl-containing intermediary occurs readily and causes loss of efficacy of GTN. This is clinically important with GTN patches and with longer acting organic nitrates (e.g. isosorbide dinitrate), and is called tolerance. Tolerance can be avoided by using these preparations intermittently, for example by omitting the evening dose in patients who do not experience angina at night. sodium nitroprusside
Nitric oxide mediates the action of nitrovasodilators (GTN, sodium nitroprusside). It combines avidly with a heme group in guanylyl cyclase - cGMP - sequestration of free calcium ions within sarcoplasmic reticulum, thereby relaxing smooth muscle. NO can also inhibit platelet function Under physiological conditions NO (synthesized from L-arginine) is the “EDRF“ responsible for the resting vasodilator tone present in human resistance arterioles under basal conditions. Nitrovasodilator drugs provide NO in anendothelium-independent manner, and hence are effective even if endothelial function is severely impaired, as in many patients with coronary artery disease.
Hemodynamic effects TNT is relatively selective for venous rather than arteriolar smooth muscle. Venodilatation reduces cardiac preload. reduced ventricular filling and hence in ventricular chamber diameter.Ventricular wall tension is directly proportional to chamber diameter (the Laplace relation), so wall tension is reduced by TNT which thereby reduces cardiac work and oxygen demand. The mild reduction in arterial tone reduces afterload and thus also reduces myocardical oxygen demand. In addition, coronary blood flow improves due to the decreased left ventricular end-diastolic pressure (improves forward flow in the coronaries) + NO-mediated coronary artery relaxation. Nitrates also relax some non-vascular smooth muscles, and therefore sometimes relieve the pain of esophageal spasm and biliary or renal colic causing potential diagnostic confusion.
Adverse effects As mentioned above GTN and the other organic nitrates are generally very safe drugs, although they can cause hypotension in patients with diminished cardiac reserve. Headache is a common problem. Another problem with continuous rather than intermittent therapy with organic nitrates is the occurrence of tachyphylaxis. This is minimized by removing the patch at night, or omit night dose - regimen (2 - 1 - 0).
Indications: • CAD • pulmonary edema due to left ventricular failure • hypertension emergency • Contraindications: • hypotension • increase intracranial pressure • aortal stenosis
b-ADRENOCEPTOR ANTAGONISTS The main uses of b-blockers in patients with ischemic heart disease are in prophylaxis of angina, and in reducing the risk of sudden death or reinfarction following myocardial infarction ("secondary prevention"). In addition, b-blockers are used in treating hypertension, cardiac arrhythmias, in patients with essential tremor and to suppress symptoms of hyperthyroidism before more specific therapy has time to work (risk factors for CAD).
Mechanism of action b-Adrenoceptors are linked via stimulatory G-proteins to adenylyl cyclase, so endogenous b-agonists (noradrenaline or adrenaline) increase cytoplasmic cAMP. In cardiac tissue cAMP: force of contraction and heart rate is arrhythmogenic in arteriolar vascular smooth muscle - vasodilatation in the juxta-glomerular cells in the kidney causes renin release in airways smooth muscle causes relaxation. b-Blocking drugswork by competing with endogenous noradrenaline and adrenaline and thereby reduce their b-receptor-mediated effects.
Pharmacological effects Sympathetic stimulation increases myocardial oxygen consumption. Increased sympathetic activity is associated with exercise, emotion and going out in the cold, all of which precipitate angina, and in most patients b-adrenoceptor blockade reduces the frequency of attacks. Conversely, patients in whom coronary artery spasm is particularly important may paradoxically deteriorate if treated with b-blockers because of unopposed a-adrenoceptor-mediated coronary vasoconstriction, although this is uncommon. Studies in angina patients indicate that most b-blockers are similarly effective despite pharmacological differences.
Adverse effects and contraindications Adverse effects are also similar among b-receptor antagonists: all such drugs can precipitate cardiac failure, obstructive airways disease is similarly worsened by all such drugs, and relatively contraindicates their use. heart block (unless the patients is already paced) should be avoided if possible in patients with peripheral vascular disease and Raynaud´s disease. diabetes (Symptoms of hypoglycemia may be masked.) abrupt discontinuation of treatment with b-blockers sometimes provokes a rebound increase in frequency and severity of angina and instances of myocardial infarction have been documented in this setting - upregulation of b-receptors. It occurs most commonly in those patients who experienced the greatest relief when b-blockers were started and who continue strenuous activity during the first 1-2 days after stopping.
Pharmacokinetics Propranolol - first b-blocker, nonselective, has substantial and highly variable presystemic metabolism (CYP2D6), making dose titration particularly important. Atenolol and/or metoprolol have largely replaced propranolol - "cardioselective" - need less frequent dosing, and the clinically useful range of doses is much less wide than that of propranolol, making them rather easier to use. Atenolol is eliminated by the kidneys and is excreted largely unchanged in the urine, whereas metoprolol is inactivated by hepatic metabolism.
CALCIUM ANTAGONISTS - for prophylaxis of angina, and possibly to provide secondary prevention following subendocardial myocardial infarction. In addition they are used to treat hypertension, supraventricular tachycardia, Raynaud´s disease and (in the case of nimodipin) to prevent cerebral vasospasm following subarachnoid hemorrhage.
Mechanism of action inhibits the passage of calcium ions through voltage-dependent L-type calcium channels in cell membranes in the heart and vascular smooth muscle as well as some other excitable tissues. Ca2+ channels open more slowly "slow" channels (compare to Na). In heart: contribute to the membrane current during the plateau phase of the cardiac action potential, slow initial depolarization SA and AV nodes.
There are several chemically distinct classes of calcium antagonists: dihydropyridines, e.g. nifedipine, amlodipine, nicardipine phenylalkylamines, e.g. verapamil benzothiazepines, e.g. diltiazem All are absorbed from the gastrointestinal tract and metabolized in the liver, inactive metabolites being excreted in the urine.
Hemodynamic and electrophysiologic effects of calcium antagonists Coronary dilatation Peripheral dilatation Negative inotropic AV conduction Heart rate blood pressure Sinus node depression Cardiac output + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + + Nifedipine Diltiazem Verapamil
Pharmacological effects Relaxation of coronary vascular smooth muscle may be useful in patients with coronary vasospasm. arteriolar dilatation - afterload. myocardial contractility (negative inotropic effect). This is partly offset by reduced afterload. All calcium channel antagonists have a negative inotropic effect; nicardipine is possibly least harmful in this regard, while verapamil is the most markedly negatively inotropic. Verapamil and diltiazem depress the cardiac conducting system. sinus node automaticity usually produces a mild resting bradycardia. conduction through the AV node accounts for antiarrhythmic effects Lack of reflex tachycardia is useful in patients with unstable coronary artery disease (e.g. following subendocardial myocardial infarction).
Adverse effects and contraindications The main contraindication - cardiac failure, because of their negative inotropic effect - . most likely when verapamil (or another calcium channel blocking drug) is used intravenously, especially in patients recently treated with b-antagonists. In contrast to b-blockers, calcium antagonists may be given safely to patients with asthma, chronic bronchitis, peripheral arterial disease or diabetes. Verapamil and diltiazem must not be given to patients with heart block or bradycardia.
Flushing and headache related to vasodilatation - most marked at peak plasma concentration (less troublesome in patients treated with amlodipine, which has a long half-life and consequently a relatively stable plasma concentration profile) Ankle swelling is another common effect of the dihydropyridine calcium channel blocking drugs. (uncommon with verapamil. Verapamil frequently causes constipation, which may be severe, because of its effect on calcium channels in the gut. Occasionally patients experience increased frequency of micturition, partly because of a mild diuretic effect and perhaps also partly due to an effect on muscle in th bladder.
Interactions. pharmacodynamic interaction with b-blockers (and presumably also with other negative inotropes), verapamil has a clinically significant pharmacokinetic interaction with digoxin, increasing its plasma concentration and potentially causing toxicity. When chronic treatment with verapamil is started in a patient previously stabilized on digoxin it is therefore prudent to halve the digoxin dose when possible and to check plasma digoxin after around a week.
ASPIRIN The use of aspirin depends on its effects on platelet function. improves the rate of survival in patients with AMI and reduces the risk of MI in patients with stable and unstable angina, and after recovery from myocardial infarction. (It is not, however, recommended generally as prophylaxis in asymptomatic men, because of adverse effects). patients with transient cerebral ischemic attacks in whom it reduces the risk of stroke. the risk of thromboembolism in patients with atrial fibrillation and following valve replacement. inhibition of fatty acid cyclooxygenase anti-inflammatory, antipyretic and mild analgesic effects in addition to its effect on platelet function, which is evidenced by a mild prolongation of bleeding time.
ANGINA OF EFFORT Nitrate + b-blocker + aspirin UNSTABLE ANGINA - every new angina (4 weeks), worsening of existing angina, episodes of angina at rest . - no signs of AMI (no Q wave, cardiospecific enzymes are below 200% of normal values) VASOSPASTIC ANGINA Calcium channel-blocking + nitrates
Newly developed angina nitrate + b-blocking dg. + aspirin; ev. Ca-channel blocking dg. stabilisation progresion ergomethry, 24-h ambulatory ECG (Holter) Admision to hospital heparine i.v., ev. ASA nitrate i.v. b-block, Ca block. spec. indications progresion invasive examination with possible revascularization (angioplasty) or fibrinolysis; coronary bypass grafts
MYOCARDIAL INFARCTION intensive care unit. General nursing: - bed rest - 24 h. - i.v. line keep vein open - 5% dextrose - min. 8-h without food and drink - monitoring of blood pressure every 15 min for 8 hr Investigations: - ECG, creatine kinase (CK) - measurement of CK-MB isoenzyme levels, every6 hr for 24 hr - chest X-ray
Analgesics - Morphine, Pethidine or fentanyl + dihydrobenzperidol (! vagal stimulation). Sedatives - diazepam i.v. at bedtime Nasal oxygen - 2-4 l/min if needed Stool softener Fibrinolytics - t-PA or streptokinase Antikoagulants - heparine (i.v. or s.c.) Beta-blocking drugs - must add unless COI i.v. (metoprolol 5 mg i.v., repeat after 10 min.) CAVE contraind. (heart failure, systolic BP below 100, bradycardia) ACE inhibitors- patients with EF < 0.4. Nitrates i.v. - (TNT 5g/min) especially in patients with hypertension, pain non-responding to analgesics. CAVE hypotension, infarct of right ventricle (venodilatation)