Download
1 / 20
200 likes | 404 Views
Tibial Plafond Fracture w/ C-Diff. Case 12.

E N D
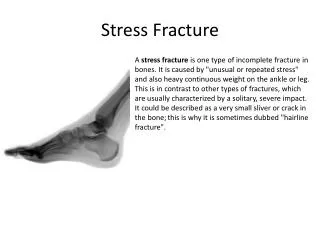
Case 12 • Lavonia is a 49 yo RN in the hospital where you work. She slipped on a wet floor in a patient’s room and sustained a comminuted and displaced tibial plafond fracture. She was hospitalized for the repair, post-op she developed a fever, after 8 days of diarrhea clostridium difficile was cultured.
Fracture Management • Fracture Detection • Cardinal Signs of Inflammation • Erythema • Swelling • Pain • Heat • Loss of Function (unable to weight bear) • Pain on palpation • Positive Thump Test
Fracture Management • Fracture Detection realistically: • Tibial Plafond are normally caused by high energy impacts such as MVAs or falls from heights • Most likely the pt. will be admitted to the ER before coming to PT
Fracture Management • Fracture Characteristics: • Tibial plafond is the horizontal weightbearing surface of the distal tibia • Isolated fractures of the medial and lateral malleoli may or may not be present • Plafond is sometimes confused with the tibial pilon which is the supramalleolar portion of the distal tibia • Plafond fractures may or may not extend up into the pilon • Due to the usual mechanism of injury, these fractures are often comminuted and displaced
Fracture Management • Images here
Fracture Management • Orthopaedic Objectives: • Restoration of articular surface is vital to prevent arthritis and to allow pain-free function • Restore tibial and fibular length to promote normal anatomic alignment and prevent leg length discrepancy • Reconstruction of any connective tissue damage such as the distal tibiofibular syndesmosis
Fracture Management • Stabilization Options: • ORIF • External Fixation • Casting • Arthrodesis
Fracture Management • ORIF • Primary choice for plafond stabilization, Providing best realignment of articular surfaces greatly improving long-term prognosis (Hoppenfeld, 2000) • Primary healing without callus formation sometimes with the assist of a bone graft • Allows for early motion • A protective cast or splint is used postoperatively
Fracture Management • External Fixation • Indicated when soft-tissue injury prevents ORIF • Allows for the care of muscle flaps or skin grafts if necessary • Articular restoration is not as complete as with ORIF • Secondary bone healing with callus formation
Fracture Management • Casting • Indicated for non/minimally displaced fractures with little or no impaction • Does not allow for early motion • Arthrodesis • Indicated when significant comminution prevents successful ORIF • Treatment of last resort
Fracture Complications • Associatied ligamentous and tendonous damage due to typical mechanisms of injury • Often disruption of the ligamentous complex around the ankle joint rendering it unstable. • Unstable ankle joint can lead to abnormal stress and strain on the articular surface of the joint increasing likelyhood for developing arthritis • Predispose person to chronic ankle sprains
Complications • Monitor for compartment syndrome especially with closed reduction and casting • Fasciotomies may be required to reduce pressure to prevent ischemia and protect the neuro-vascular structures • Symptoms of compartment syndrome: • Monitor for signs of RSD • Signs of RSD
Fracture Rehabilitation • Day one to one week • No stability of fracture • Monitor for compartment syndrome and infection of surgical site. With ORIF in particular monitor for sloughing or necrosis of tissue. • With ORIF Pt should be in a well-padded nonconstricting splint that keeps ankle in neutral position. Should be instructed to ice and elevate leg to help control swelling. • All types of stabilization should be non-weight bearing • ORIF may begin AROM of the ankle as tolerated, AROM of the MTP joints and knee joints
Fracture Rehab Days 1-7 • Exam • monitor for compartment syndrome, cast fit, and infection of surgical site • WB status: all pts should be non-weight bearing • ROM • ORIF may begin AROM of the ankle as tolerated, also AROM of the MTPs and knee joint • Cast and external fixation may begin AROM of the MTPs and knee joint • Strength • Quad sets as tolerated • Functional Activities • Pts should be taught to perform stand-pivot transfers with assistive devices • Crutch training-using non-weight bearing two point gait
Fracture Rehab Days 7-14 • Exam • Continue to monitor surgical site, cast fit, and signs of RSD • WB • Non-weight bearing due to instability of fracture • ROM • ORIF AROM of ankle, knee, and MTPs • Non-rigidly fixed AROM of knee and MTPs • Strength • Isometric DF/PF and quad sets for rididly fixed fractures • No strengthening exercises for non-rigidly fixed fractures • Functional Activities • Same as days 1-7
Fracture Rehab Wks 4-6 • Exam • Monitor for signs of RSD • Pts in long leg-cast will typically have cast for radiographic exam to check status of fracture union. Expect stiffness, decreased ROM and strength • WB status/Bone Healing • Fracture is now usually stable with callus formation. Callus is weak especially with torsional forces. • Non-weightbearing • ROM • Rigid fixation: same as previous • Non-rigid fixation: add ankle ROM as immobilization devices allow • Strength • Rigid fixation: same as previous • Non-rigid fixation: add gentle DF and PF isometrics in cast. No resistive exercises to long flexors or extensors of toes. Continue quad strengthening • Functional Activity • Same as previous
Fracture Rehab Wks 6-8 • Exam • All fractures should be examined radiographically for loss of reduction and healing status • WBing/Bone Healing • Fracture usually stable with bridging callus but torsional strength remains limited • Non/minimally displaced showing good callus formation may begin partial wbing • Those with significant displacement or those with bone grafts should continue strict non-weightbearing • ROM • Rigid fixation: AROM in all planes of ankle and subtalar jt • Non rigid fixation: ROM of ankle and knees as immobilization allows. Cont. AROM of MTPS • Strength • Rigid fixation: Cont. isometrics to dorsiflexors and plantarflexors. Add knee and hip isometrics as indicated. No resistive exercise to long toe flexors/extensors. Cont. quad isotonic strengthening. • Non Rigid: Cont. isometric dorsiflexion and plantarflexion as allowed by cast. Cont quad strengthening. No resistive exercise to long toe extensors/flexors. • Functional Activity • Rigid: Begin 3-point gait with crutches and partial wbing during transfers • Non-rigid: Remain non-wbing
Fracture Rehab Wks 8-12 • Exam • Continue monitoring for RSD and surgical site incision • Weightbearing/Healing Status • Cont. partial weightbearing as before • With comminuted fractures begin toe-touch weightbearing as tolerated • Bridging callus becoming laminar bone and ligamentous healing across ankle jt should be well established • ROM/Strength • Rigid: Aggressive resistive exercise in all planes at the ankle and subtalar jt • Non-rigid: Begin A/PROM and pain-free resistive exercises at the ankle and subtalar jts • Functional Activity • Rigid: Progress from partial to full weightbearing • Non-rigid: Partial weightbearing as tolerated
Fracture Healing • Long Term Considerations: