Download
1 / 26
270 likes | 486 Views
Pituitary tumor in pregnancy . 報告者: R1 張嘉珮 指導教師:楊明智 醫師 日期: 980227. In pregnancy the normal pituitary gland enlarges . This is mainly due to an increase in the number and size of the lactotrophic cells. This increase in pituitary size does not result in visual field changes.

E N D
Pituitary tumor in pregnancy 報告者:R1 張嘉珮 指導教師:楊明智 醫師 日期:980227
In pregnancy the normal pituitary gland enlarges. This is mainly due to an increase in the number and size of the lactotrophic cells. This increase in pituitary size does not result in visual field changes
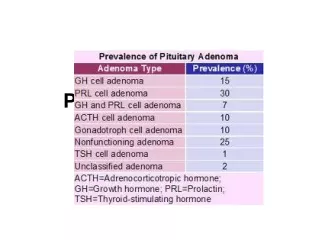
Several distinct types of tumors can occur in the pituitary gland. Pituitary adenomas derived from adenohypophyseal cells are the most common in pregnancy.
Pituitary adenomas are often classified on the basis of size Microadenomas < 10mm in diameter Macroadenomas > 10mm in diameter The risks to the mother adenoma size The potential risks to the fetus treatment Gonzalez, JG, Elizondo, G, Saldivar, D, Nanez, H. Pituitary gland growth during normal pregnancy: an in vivo study using magnetic resonance imaging. Am J Med 1988; 85:217.
Risks to the mother Increase in adenoma size cause neurologic symptoms, most importantly visual impairment Theoretical basis -- hyper-estrogenemia causes lactotroph hyperplasia
Microadenomas The risk of a clinically important increase in the size of a lactotroph microadenoma during pregnancy is small
Macroadenomas The outcome is substantially worse in women with macroadenomas In a 1979 survey, 46 women with lactotroph macroadenomas were followed during 56 pregnancies. Symptoms occurred in 20 (36 percent): headache : 5 headache and visual impairment :14 diabetes insipidus: 1 Gemzell, C, Wang, CF. Outcome of pregnancy in women with pituitary adenoma. Fertil Steril 1979; 31:363.
Potential risks to the fetus One potential risk to the fetus results from dopamine agonisttreatment of hyperprolactinemia in order to permit ovulation and thereby conception spontaneous abortions , extrauterine pregnancies, and minor or major malformations Ricci, E, Parazzini, F, Motta, T, et al. Pregnancy outcome after cabergoline treatment in early weeks of gestation. Reprod Toxicol 2002; 16:791.
TREATMENT DURING PREGNANCY When a dopamine agonist is needed to lower the serum prolactin concentration to permit ovulation, we recommend bromocriptinerather than cabergoline, because of the greater certainty that it does not cause birth defects Casanueva, FF, Molitch, ME, Schlechte, JA, et al. Guidelines of the Pituitary Society for the diagnosis and management of prolactinomas. Clin Endocrinol (Oxf) 2006; 65:265.
Early administration does not harm Bromocriptine during the first monthof pregnancy does not harm -- sufficient data are available however, insufficient data are available about the use of bromocriptine later in pregnancy Schade, R, Andersohn, F, Suissa, S, et al. Dopamine agonists and the risk of cardiac-valve regurgitation. N Engl J Med 2007; 356:29.
Microadenomas (1) Risk is very small Should not be a deterrent to becoming pregnant Bromocriptine or cabergoline will likely be effective Should be given bromocriptine or cabergoline before pregnancy in whatever dosage is necessary Bromocriptine should be discontinued as soon as pregnancy has been confirmed Turkalj, I, Braun, P, Krupp, P. Surveillance of bromocriptine in pregnancy. JAMA 1982; 247: 1589
Microadenomas (2) During the pregnancy, the woman should be seen every three monthsand asked about headaches and changes in vision. If no symptoms occur, serum prolactin can be measured two months after delivery or cessation of nursing, and if it is similar to the pretreatment value, the drug can be resumed.
Macroadenomas (1) Relatively higher risk of clinically important tumor enlargement during pregnancy If the adenoma does not elevate the optic chiasm, treatment with bromocriptine or cabergoline should reduce the chance of enlargement during pregnancy Ahmed, M, Al-Dossary, E, Woodhouse, NJY. Macroprolactinomas with suprasellar extension: effect of bromocriptine withdrawal during one or more pregnancies. Fertil Steril 1992; 58:492.
Macroadenomas (2) Once adenoma has shrinked, the woman can attempt to become pregnant; the dopamine agonist should be discontinued when pregnancy has been confirmed. Monitoring during pregnancyshould be similar to that described above for women with microadenomas
If the adenoma has enlarged to a degree that could account for the symptoms, the woman should be treated with bromocriptine throughout the remainder of the pregnancy. Konopka, P, Raymond, JP, Merceron, RE, Seneze, J. Continuous administration of bromocriptine in the prevention of neurological complications in pregnant women with prolactinomas. Am J Obstet Gynecol 1983; 146:935.
If the adenoma does not respond to bromocriptine, cabergoline may be successful If cabergoline is not successful, transsphenoidalsurgery could be considered Liu, C, Tyrrell, JB. Successful treatment of a large macroprolactinoma with cabergoline during pregnancy. Pituitary 2001; 4:179.
Surgery for persistent visual symptoms in the third trimestershould be deferred until delivery if possible If the adenoma is very large or elevates the optic chiasm, pregnancy should be strongly discourageduntil the adenoma has been treated by transsphenoidal surgery
summary A perceived a change in visionshould be assessed by a neuroophthalmologist MRI should be performed if an abnormality consistent with a pituitary adenoma is confirmed.
Pregnancy should also be discouraged in a woman whose macroadenoma is unresponsive to bromocriptine and cabergoline, even if it is not elevating the optic chiasm, until the size has been greatly reduced by transsphenoidal surgery, because medical treatment would not likely be effective if the adenoma enlarges during pregnancy.
Breast feeding Not increase the risk of lactotroph adenoma growth Dopamine agonist treatment should be withheld until breastfeeding is completed. Breastfeeding is contraindicated in women who have neurologic symptoms at the time of delivery (suggesting tumor growth), because they should be treated with a dopamine agonist.