Download
1 / 40
590 likes | 1.8k Views
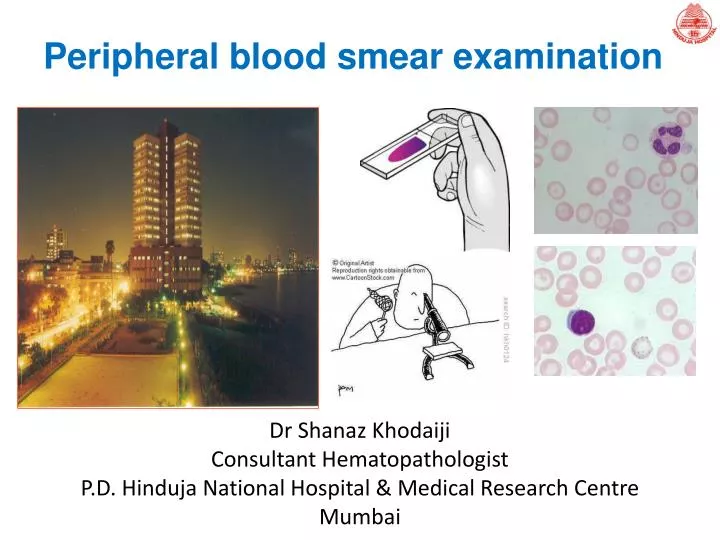
Peripheral blood smear examination. Dr Shanaz Khodaiji Consultant Hematopathologist P.D. Hinduja National Hospital & Medical Research Centre Mumbai. CBC on automated analyzers. Hemogram: measured and calculated parameters Histograms: size distribution of WBC, RBC and Plt

E N D
Peripheral blood smear examination Dr Shanaz Khodaiji Consultant Hematopathologist P.D. Hinduja National Hospital & Medical Research Centre Mumbai
CBC on automated analyzers Hemogram: measured and calculated parameters Histograms: size distribution of WBC, RBC and Plt Cytogram: WBC differential Flagging for abnormalities necessitates a manual PBS review
A well made peripheral smear is thick at one end and progressively thinner at the opposite end. The "zone of morphology" (area of optimal thickness for light microscopic examination) should be at least 2 cm in length. The smear should occupy the central area of the slide and be margin-free at the edges
PBS examination requires a systematic approach in order to gather all possible information. In addition, all specimens must be evaluated in the same manner, to assure that consistent information is obtained.
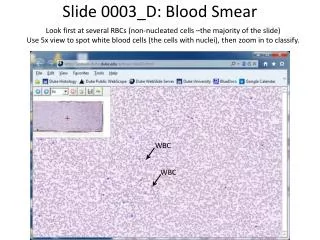
PBS examination - preliminary • The examination starts with • Macroscopic view to evaluate the quality of the smear • The microscopic analysis begins on lower power (10x), primarily to assess cellular distribution, staining quality, and to select an area where the RBCs are barely touching each other. This area is used to assess the cellular elements on higher magnification. • On hi-dry (40x), the slide is principally scanned to obtain a WBC estimate. All of the detailed analysis of the cellular elements is performed using high power or oil immersion.
Scanning technique for WBC differential count and morphologic evaluation (a) Ten microscopic fields are examined in a vertical direction from bottom to top or top to bottom (b) The slide is horizontally moved to the next field (c) Ten microscopic fields are counted vertically. (d) The procedure is repeated until 100 leukocytes have been counted
PBS examination - final • This final microscopic examination is performed at 50x or 100x oil immersion and includes: • A WBC differential • The identification of abnormal leukocytes • Assessment of RBC morphology • The number and morphology of the platelets • The identification of intra- and extra-cellular elements • Assessment of any organisms present
Hematology analyzer and PBS • Microscopic examination of the peripheral blood is used to supplement information provided by CBC analyzers. • Hematology analyzers provide accurate quantitative information about blood cells and can identify abn cells • In addition to providing cell counts and graphical displays these instruments also provide a warning flags • The instrument operator reviews the information from each specimen and decides if smear preparation and light microscopy are necessary. • If not, the information is released to the clinician.
WBC estimation on peripheral smear • A fairly accurate estimate of the WBC count (cells/mL) can be obtained by counting the total number of leukocytes in ten 50X microscopic fields, dividing the total by 10, and multiplying by 3000. These estimates should approximate that obtained by the cell analyzer. If the estimate does not match the automated cell count, obtain the original blood specimen, confirm patient identity, repeat the automated analysis, and prepare a new smear.
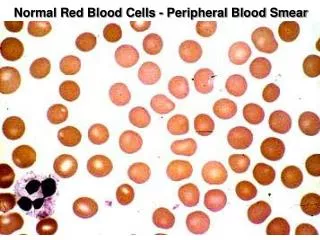
Morphologic Evaluation of Red Blood Cells • Round to very slightly ovoid cells with a mean diameter of approximately 7 µ • A central pale area - central pallor approximately 1/3 the diameter of the cell • It is approximately the same size as the nucleus of a mature lymphocyte. • Any deviation in size, volume, or shape represents an abnormal red blood cell.
Elliptocytes or ovalocytes Ovalocytes are due to abnormal membrane cytoskeleton found in hereditary elliptocytoisis
Tear drop cells / dacrocytes Tear drop shaped red cells or dacryocytes are seen when there is extramedullary erythropoiesis or with marrow disorders or marrow infiltration, such as myelofibrosis or metastatic carcinoma.
Acanthocytes Acanthocytes or spur cells, are spherical cells with blunt-tipped or club-shaped spicules of different lengths projecting from their surface at irregular intervals. (Echinocytes, or crenated red cells, in contrast, have shorter, sharp to blunt spicules of uniform length which are more evenly spaced around their periphery).
Schistocyte – fragmented RBC • normal newborns • bleeding peptic ulcer • Aplastic Anemia • pyruvate kinase def • Vasculitis • Glomerulonephritis • renal graft rejection • severe burns • iron deficiency, thalassemia • Mechanical damage to RBCs from fibrin deposits • DIC • MAHA • TP • prosthetic heart valves • severe valvular stenosis • malignant hypertension • march hemoglobinuria • myelofibrosis hypersplenism
Some specific hemolyic anemias Mechanical HAs: RBC are injured by excess physical trauma as they circulate in the blood vessels Cardiac hemolytic anemias – artificial heart valve MAHA - due to thrombosed vessels or fibrin strands as in DIC, TTP, malignancy Hallmark: Presence of schistocytes in the PB
HA due to red cell enzyme defects – bite or blister cells G6PD deficiency Sex linked transmission Presents as hemolysis after drug intake, infections Common drugs – antimalarials, acetanilide dapsone furantoin Lab diagnosis – screening, quantitative tests Pyruvate kinase deficiency – uncommon Lab diagnosis – fluorescent spot test
Alder-Reilly anomaly Large, coarse, dark purple, azurophilic granules that occur in the cytoplasm of most granulocytes. These are characteristically found in the Alder-Reilly anomaly and in patients with mucopolysaccharidoses
Chédiak-Higashi Chédiak-Higashi granules are very large red or blue granules that appear in the cytoplasm of granulocytes, lymphocytes, or monocytes in patients with the Chédiak-Steinbrinck-Higashi syndrome. It is a rare autosomal recessive disorder
Döhle bodies Variably sized (0.1 to 2.0 um) and shaped, blue or grayish-blue cytoplasmic inclusions usually found near the periphery of the cell. Dohle bodies are lamellar aggregates of rough endoplasmic reticulum, which appear in the neutrophils, bands, and metamyelocytes of patients with infection, burns, uncomplicated pregnancy, toxic states, or during treatment with hematologic growth factors - G-CSF.
May-Hegglin anomaly Neutrophils contain small basophilic cytoplasmic granules which represent aggregated ribosomes. Leukopenia and large platelets are also found. An autosomal dominant trait, the May-Hegglin anomaly is associated with a mild bleeding tendency, but not by an increased susceptibility to infection
Neutrophilic toxic granulation Small dark blue to purple granules resembling primary granules in the cytoplasm of metamyelocytes, bands, and segmented neutrophils during inflammatory states, burns, and trauma, and upon exposure to hematopoietic growth factors. It is usually accompanied by a shift to the left and vacuolations in the cytoplasm (toxic vacuolations) and Dohle bodies.
Platelet morphology Macroplatelets
Disadvantages of the Peripheral Blood Smear • Provides information that cannot be obtained from automated cell counting. However, some limitations are: • Experience is required to make technically adequate smears. • There is a non-uniform distribution of white blood cells over the smear, with larger leukocytes concentrated near the edges and lymphocytes scattered throughout. • There is a non-uniform distribution of RBCs over the smear, with small crowded red blood cells at the thick edge and large flat red blood cells without central pallor at the feathered edge