Download
1 / 79
840 likes | 1k Views
The Art and Science of Insulin. Thomas Repas D.O. Diabetes, Endocrinology and Nutrition Center, Affinity Medical Group, Neenah, Wisconsin Member, Inpatient Diabetes Management Committee, St. Elizabeth’s Hospital, Appleton, WI

E N D
The Art and Science of Insulin Thomas Repas D.O. Diabetes, Endocrinology and Nutrition Center, Affinity Medical Group, Neenah, Wisconsin Member, Inpatient Diabetes Management Committee, St. Elizabeth’s Hospital, Appleton, WI Member, Diabetes Advisory Group, Wisconsin Diabetes Prevention and Control Program Website: www.endocrinology-online.com
Overview • Goals and Purpose of Insulin Therapy • Barriers to the use of Insulin • Current Concepts in Insulin Therapy • Basal/Bolus Insulin • Sliding Scales • Insulin Pump Therapy • Future of Insulin • Conclusion !
Purpose of Insulin Therapy • Prevent and treat fasting and postprandial hyperglycemia • Permit appropriate utilization of glucose and other nutrients by peripheral tissues • Suppress hepatic glucose production • Prevent acute complications of uncontrolled diabetes • Prevent long term complications of chronic diabetes
The Goal of Insulin Therapy:Attempt to Mimic Normal Pancreatic Function Schade, Skyler, Santiago, Rizza, “Intensive Insulin Therapy,” 1993, p. 131.
WHAT!? Did you say INSULIN?! Barriers to the Use of Insulin
Patient Concerns About Insulin • Fear of injections • Perceived significance of need for insulin • Worries that insulin could worsen diabetes • Concerns about hypoglycemia • Complexity of regimens
Help Patient Accept and Prepare for Insulin Therapy • Address patient concerns • Dispel fear by countering misconceptions • Review rationale for insulin use • Explain that insulin • Can be incorporated into lifestyle • Causes only modest weight gain • Is a common course of treatment for this progressive disease • Promise patient support and close follow-up • Monitoring can prevent hypoglycemia • Today’s technology can facilitate daily injections and readings
Barriers to Insulin Therapy : Common Medical Concerns Insulin therapy in type 2 diabetes might cause: • Worsening Insulin Resistance? • More Cardiovascular Risk? • Weight Gain ? • Hypoglycemia? 6-8
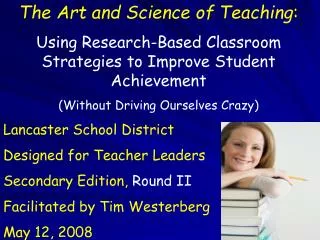
Insulin Sensitivity in Glucose Clamp Studies:Improved by Insulin Treatment Baseline After Insulin 100 87 80 80 67 57 60 53 Glucose Disposal % of Matched Control Values 40 40 20 0 Scarlett Andrews Garvey Scarlett, et al. Diabetes Care. 1982;5:353-363; Andrews, et al. Diabetes. 1984;33:634-642; Garvey, et al. Diabetes. 1985;34:222-234. 6-9
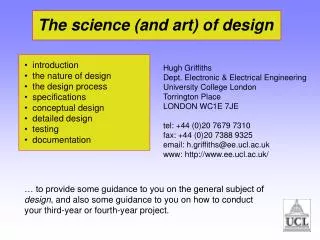
Standard treatment Cardiovascular RiskMortality After MI Reduced by Insulin Therapy in the DIGAMI Study IV Insulin 48 hours, then 4 injections daily .7 .7 All Subjects Low-risk and Not Previously on Insulin (N = 272) (N = 620) .6 .6 Risk reduction (51%) Risk reduction (28%) .5 .5 P = .011 P = .0004 .4 .4 .3 .3 .2 .2 .1 .1 0 0 0 1 2 3 4 5 0 1 2 3 4 5 Years of Follow-up Years of Follow-up Malmberg, et al. BMJ. 1997;314:1512-1515. 6-11
Reassurance About Common Concerns Insulin Therapy in Type 2 DM • Improves Insulin Sensitivity by Reducing Glucotoxicity • Reduces Cardiovascular Risk • Causes Modest Weight Gain • Rarely Causes Severe Hypoglycemia • Patients fears and concerns can be addressed by education 6-15
Comparison of Human Insulins and Analogues Insulin Onset of Duration ofPreparations Action Peak Action Lispro/Aspart 5-15 minutes 1-2 hours 3-5 hours Human Regular 30-60 minutes 2-4 hours 4-8 hours Human NPH/Lente 1-4 hours 4-12 hours 10-20 hours HumanUltralente 6-8 hours Unpredictable 16-20 hours Glargine 2-3 hours Flat ~24 hours The time course of action of any insulin may vary in different individuals, or at different times in the same individual. Because of this variation, time periods indicated here should be considered general guidelines only. 6-22
Twice-daily Split-mixed Regimens Regular NPH Insulin Effect B L S HS B 6-23
Multiple Daily Injections (MDI)NPH + Regular NPH at AM and HS + Regular AC NPH at HS + Regular AC Regular Regular NPH NPH Insulin Effect Insulin Effect B L S HS B B L S HS B 6-24
Multiple Daily Injections (MDI)Ultralente + Regular Regular Ultralente Insulin Effect B L S HS B 6-25
Limitations of Human Regular Insulin • Slow onset of action • Requires inconvenient administration: 20 to 40 minutes prior to meal • Risk of hypoglycemia if meal is further delayed • Mismatch with postprandial hyperglycemic peak • Long duration of activity • Up to 12 hours’ duration • Increased at higher dosages • Potential for late postprandial hypoglycemia 6-26
The Basal/Bolus Insulin Concept • Basal Insulin • Suppresses glucose production between meals and overnight • Nearly constant levels • 50% of daily needs • Bolus Insulin (Mealtime or Prandial) • Limits hyperglycemia after meals • Immediate rise and sharp peak at 1 hour • 10% to 20% of total daily insulin requirement at each meal Ideally, for insulin replacement therapy, each component should come from a different insulin with a specific profile 6-20
Insulin and Glucose Patterns: Normal and Type 2 Diabetes Normal Type 2 Diabetes Glucose Insulin 400 120 100 300 80 mg/dL U/mL 200 60 40 100 20 0600 1000 1400 1800 2200 0200 0600 0600 1000 1400 1800 2200 0200 0600 B L S B L S Time of Day Time of Day Polonsky, et al. N Engl J Med. 1988;318:1231-1239. 6-17
Rapid-acting Analogues: Clinical Features • Insulin profile more closely mimics normal physiology • Convenient administration immediately prior to meals • Faster onset of action • Limit postprandial hyperglycemic peaks • Shorter duration of activity • Reduced late postprandial hypoglycemia • But more frequent late postprandial hyperglycemia • Need for basal insulin replacement revealed 6-27
Rapid-acting Insulin Analogues: Lispro and Aspart 400 500 Aspart Lispro 450 350 400 300 350 250 300 250 200 Plasma Insulin (pmol/L) Plasma Insulin (pmol/L) Regular 200 150 Human 150 Regular 100 100 Human 50 50 0 0 0 30 60 90 120 150 180 210 240 0 50 100 150 200 250 300 Time (min) Time (min) Meal SC injection Meal SC injection Heinemann, et al. Diabet Med. 1996;13:625-629; Mudaliar, et al. Diabetes Care. 1999;22:1501-1506. 6-28
Lispro Lispro NPH NPH Insulin Effect Insulin Effect B L S HS B B L S HS B Multiple Daily Injections (MDI)NPH + Mealtime Lispro NPH at AM and HS + Lispro AC NPH at HS + Lispro AC 6-29
Limitations of Human NPH, Lente, and Ultralente • Do not mimic basal insulin profile • Variable absorption • Pronounced peaks • Less than 24-hour duration of action • Cause unpredictable hypoglycemia • Major factor limiting insulin adjustments • More weight gain 6-30
The Quest for Basal Insulin Replacement Mealtime Lispro + NPH and NPH at HS Lispro NPH Insulin Effect B L S HS B Bolli, et al. Diabetologia. 1999; 42:1151-1167. 6-31
The Ideal Basal Insulin . . . • Mimics normal pancreatic basal insulin secretion • Long-lasting effect around 24 hours • Smooth, peakless profile • Reproducible and predictable effects • Reduced risk of nocturnal hypoglycemia • Once-daily administration for convenience 6-32
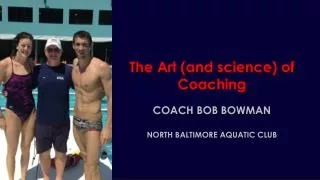
n = 20 T1DM Mean ± SEM SC insulin 4.0 3.0 2.0 1.0 0 24 20 16 12 8 4 0 NPH Ultralente mg/kg/min mol/kg/min CSII µ Glargine 0 4 8 12 16 20 24 Time (h) Profiles of Various Basal Insulins SC=subcutaneous; CSII=continuous subcutaneous insulin infusion Lepore M et al. Diabetes. 2000;49:2142-2148.
Long-Acting Insulins: Ultralente and Glargine • Ultralente • Injected once or twice daily • Onset within 6–8 hours • Peak effect within 10–20 hours • Glargine • 24-hour, long-acting recombinant human insulin analogue has no peak • Cannot be diluted or mixed with other insulins or solutions • Administered once daily • In combination therapy, glargine given at bedtime; rapid- or short-acting given during the day
Glargine vs NPH Insulin in Type 1 DiabetesAction Profiles by Glucose Clamp 6 5 4 NPH Glucose Utilization Rate (mg/kg/h) 3 2 Glargine 1 0 0 10 20 30 Time (h) After SC Injection End of observation period Lepore, et al. Diabetes. 1999;48(suppl 1):A97. 6-34
Bedtime Glargine vs NPH, With Mealtime Regular 4 48 Glargine NPH 3 36 ** Patients (%) 2 24 1 12 Baseline Baseline 8.5 ± 1 8.8 ± 1 11.1 ± 4 10.6 ± 4 0 0 * 1 * * 2 * HbA1c FPG Nocturnal (%) (mmol/L) Hypoglycemia *P < .01 (change from baseline to endpoint within each group)**P < .02 (compared to NPH) Rosenstock, et al. Diabetes. 1999;48(suppl 1):A100. 6-51
Bedtime Glargine vs NPH, With Mealtime Regular 48 4 Glargine NPH 36 3 ** 24 2 Patients (%) Weight (kg) 12 1 * 0 0 Nocturnal Weight Gain Hypoglycemia *P < .0007**P < .02 (compared to NPH) Rosenstock, et al. Diabetes. 1999;48(suppl 1):A100. 6-52
Insulin GlargineSummary of Completed Trials • Glucose-insulin clamp studies of Glargine vs NPH • Smooth, continuous release from injection site • Longer duration of action with effect for about 24 hours • Peakless profile • Equivalent absorption rates at various injection sites • Clinical efficacy equivalent to NPH, with significantly less nocturnal hypoglycemia 6-35
All Type 1 diabetics should be on a basal / bolus insulin regimen to control glucose while minimizing hypoglycemia 6-19
However over time, most type 2 diabetics will also need both basal and mealtime insulin to control glucose 6-19
When Oral Medications Are Not Enough • Watch for the following signs • Increasing BG levels • Elevated A1C • Unexplained weight loss • Traces of ketonuria • Poor energy level • Sleep disturbances • Polydipsia • Next steps • Make a decision to start insulin • Offer patient encouragement, not blame Remind the patient of disease progression…
Severity of Glucose Intolerance Insulin Resistance Worsens with Time Insulin Secretion Postprandial Glucose Fasting Blood Glucose Risk of Macrovascular Complications Years to Decades Typical Diagnosis of Diabetes Natural History of Type 2 Diabetes Frank Diabetes NGT IGT Normal Blood Glucose Risk of Microvascular Complications
Initiating Insulin Therapy in Type 2 Diabetes • Let blood glucose levels guide choice of insulins • Select type(s) of insulin and timing of injection(s) based on pattern of patient’s sugar (fasting, lunch, dinner, bedtime) • Choose from currently available insulin preparations • Rapid-acting (mealtime): lispro, aspart • Short-acting (mealtime): regular insulin • Intermediate-acting (background): NPH, lente • Long-acting (background): ultralente, glargine • Insulin mixtures • Provide long-acting or intermediate-acting as basal • and rapid-acting as bolus • Titrate every week Goal: to approximate endogenous insulin secretion…
Starting With Basal Insulin: Advantages • 1 injection with no mixing • Slow, safe, and simple titration • Low dosage • Limited weight gain • Effective improvement in glycemic control 6-37
Glargine at HS + Oral Agents or Mealtime Lispro TZD lispro Metformin Glargine Glargine Insulin Effect Insulin Effect B L S HS B B L S HS B 6-56
Starting with Basal Insulin • Continue oral agent(s) at same dosage (eventually stop secretegogue) • Add single, evening insulin dose (around 10 U) • Glargine (bedtime or anytime?) • NPH (bedtime) • 70/30 (evening meal) or 75/25 • Adjust dose by fasting BG • Increase insulin dose weekly as needed • Increase 4 U if FBG >140 mg/dL • Increase 2 U if FBG = 120 to 140 mg/dL • Treat to target (usually <120 mg/dL) 6-59
Advancing Bolus/ Adding Bolus Insulin • Indicated when FBG acceptable but • HbA1c not at goal and/or • Postprandial BG not at goal (<140mg/dl) • Insulin options • To Glargine, add mealtime Regular or Lispro • To bedtime NPH, add morning NPH and mealtime Regular or Lispro • To suppertime 70/30 or 75/25, add morning 70/30 or 75/25 • Oral agent considerations • Usually stop secretagogue (it is redundant to be on insulin and secretagogue) • Continue metformin and TZD for additional glycemic and other benefits 6-60
Changing from Other regimens to Basal/Bolus Insulin Total Daily Dose (~70-75% of prior insulin regimen TDD) ~50% Basal* ~50% Bolus* Usually divided into 3 premeal doses *Range: 40 to 60%