Download
1 / 27
270 likes | 343 Views
The Encore Suite maximizes the productivity of a contact center’s workforce via integrated voice and screen recording, quality management, coaching, and its Portfolio reporting and distribution package

E N D
Conflict of interest. • Medical associate director – Merck Sharp & Dohme, Mexico. • OutcomesResearch Lead
Agenda • What are we doing to select patients for aesthetic rhinoplasty? • Key points in facial analysis • Behindthescenes of rhinoplasty: pshychology of rhinoplasty.
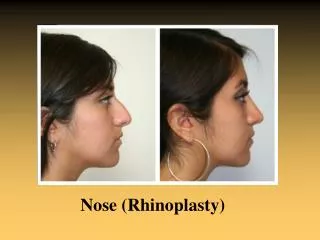
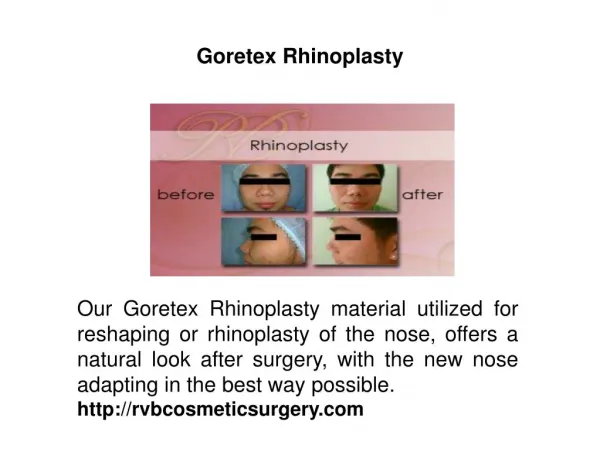
AestheticRhinoplasty • Rhinoplasty continues to rank among the most popular surgical cosmetic treatments. In 2014, nose reshaping was the second most common surgical procedure performed in the United States. • Successof rhinoplastymayvary according to the aesthetic perception of the patient as well as the preoperative status of the nose. • Nasal breathing and psychology of the patient contribute to the successful outcome.
What are wedoing to selectpatientsforaestheticrhinoplasty? • Survey of 41 Otolaryngologist and plasticsurgeonsthatperformaestheticrhinoplasty. • Questionsregardingtheirpractice and experiencewithaestheticrhinoplasty. • Descriptiveanalysis of theresults.
Results. • Years of practice: • 39.02% havebetween 5 to 10 years and more than 10 yearspracticing (78.04%) • 21.95% havelessthan 5 years of practice • Photographs • 100% use to takepreoperatoryphotographs, 93.75% bythemselves. • 84.3% use thesamebackground, 75% use thesamedistance, 34.3% special flash (avoidingshadow in thebackground), 15.6% other (same positions, light in front of patient, etc.)
Results. • Facial Analysis. • Powell & Humphrey 34.48%, thirds and fifths 79.31%, divineproportion 27.59%, other 13.79% (Gonzalez Ulloa, digital program, VIEW)
Results. • Psychologicalanalysis • 25% performananalysisbythemselves • 6.25% refer to psychologist • 68.75% do not perform any analysis. • 82.14% knowwhat body dysmorphicdisorderis.
Results • 57.14% does not document their surgical plan • Facial analysis and photographs were considered the most important aspects of preop analysis (57.14% and 78.57% respectively on a 5 point likert scale) • Pshychologicalanalysisscoredthelessimportant in 25% of the cases.
Facial analysis • Aestheticanalysisbeginswithuniversallyacceptedstandardsfor “ideal” proportions, keeping in mind individual uniqueness and howthosestandardsapply to thepatient’soverall facial structure. • Thegoals of analysis are to define external nasal deformities, predicttheunderlyinganatomicvariations, and determine theappropriatesurgicalintervention • Itdoesn´t matterwhichtype of analysisyou use, whatisimportantthatyoudocumentyour plan.
Psychology of rhinoplasty: History • The face has always been considered the personification of ones soul. It is the representation of the persons identity from the social point of view. • Facial appearance is closely tied to the self-image, self-confidence, and self-worth of the individual. • The face is the part that first enters in contact and remains the longest in interpersonal relations.
Psychology of rhinoplasty: History • Elements of appearance that have the greatest influence in interpersonal relations are attractiveness, beauty and sexual attraction. • A person is considered physically attractive if various groups of judges find him so. • This judgement is not constant, it varies in time, differs form one culture to another and is influenced by mass media, art, literature, films, publicity, etc. • With the introduction of cameras embedded in cell phones and widely acceptance of social media, facial aesthetics has been more important than ever before in the human history .
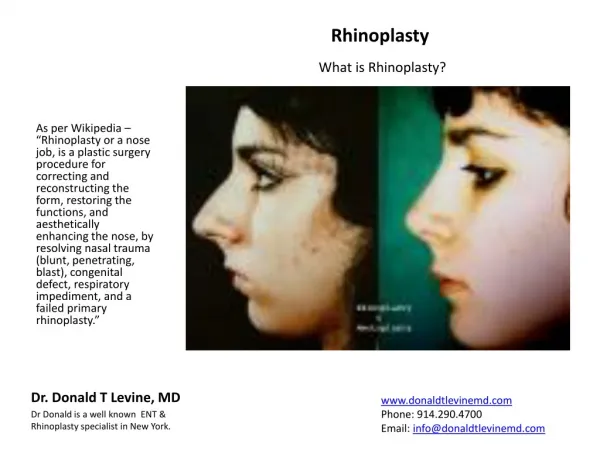
Psychology of rhinoplasty: History • The noses aspect is critical not only for the anatomy of the face, but also because this organ frequently is one of the factors that can disturb, consciously or subconsciously, our image of our body and our personality development • It has cultural, ethnic, symbolic, and psychological significance .
BUT… DOES EVERY PATIENT ASKING FOR SURGERY IS A GOOD CANDIDATE? • HOW CAN WE DIFFERENCIATE BETWEEN PATIENTS THAT WILL BENEFIT FROM SURGERY FROM THOSE WHO DON´T?
Psychology of rhinoplasty: History • Surgical advances following World War I were accompanied by enthusiastic reports of the emotional relief experienced by disfigured individuals whounderwentreconstructivesurgery. • In the 40´s and 50´s thefirstpsychiatricevaluations of peopleseekingelectivecosmeticsurgery. “WARNING” • Surgeons were cautioned of the psychopathology of the male patient, as well as of the “insatiable” surgery patient who sought out numerous cosmetic procedures in pursuit of theperfectface. • Earlyinvestigationsbasedmainlyonclinical interview, showed a 70% patientswithpsychiatricdisturbances (neuroticdepression and passive – dependentpersonality)
Clinical interview notdescribed • Diagnosticcriteria? “Markedpsychologicaldisturbance” “ deviatingfromthe normal picture” “in need of therapy”
PSYCHOLOGICAL ASSESSMENTS • Clinical Interview • Are thepatientssoughtingforthesamecosmeticprocedure, affectedbythesamepsychologicalproblem? • Isitdifferentfrom a patientsearchingfor a “type-changing” surgery (reshapingrhinoplasty) to a “restorative” surgery (facelift)? • THE MAJORITY OF COSMETIC SURGERY PATIENTS WERE PSYCHOLOGICALLY DISTURBED. • PsychometricAssessments • Manytests (Minnesota MultiphasicPersonalityInventory, BriefSymptomInventory, EysenckPersonalityInventory, etc) • Themeasuresused are notdesigned to tapthetypes of psychopatologyspecific to thesepatients.
Lesspsychopathology • No clearrelationshipbetweengivencosmeticprocedures and specificforms of psychopathology
Satisfaction • Patient’s satisfaction has been defined as the patient’s perceived improvement in well-being followingtheintervention. • Aproximately 10 to 15% of patients are notsatisfiedbyresults of cosmetic nasal surgery. • A case series of rhinoplastyrevisionshowedthat 41% of the cases, askedfortherevisionbecausetheynotedasymmetriesorirregularities in the nasal dorsum, 33% askedforrevisionbecausetheynotednotenoughcorrection of nasal deformity.
Patient Satisfaction? • A UK Department of Health systematic review identified only 9 specific instruments that demostrated adequate psychometric properties and were developed with patient input. • Patient satisfaction with their appearance is an often overlooked outcome, and able to be measured in facial aesthetics using the FACE-Q scales.
Patient reported outcomes • Patient-reported outcomes are the patients’ feedback, elicited directly from them without interpretation by the physician or others, on how they perceive the physical, mental, or social condition related to their condition or treatment. • Systematic use of PRO tools improves communication and decision making between physicians and patients and enhances patient satisfaction with care.
Bodydysmorphicdisorder (BDD) • Isone of themostcommonpsychiatricconditionsfoundin patientsseekingcosmeticsurgery. About 5% and up to 16.6% isthereported global prevalence • A study in Iranshowed a 31.5% prevalenceamongrhinoplastycandidates and 70.7% of themhadmoderate to severeforms of BDD. • 80% of plasticsurgeons in the USA reporttheywouldnotoperate a patientwith BDD, but 84% has unwillinglyoperated at leastone.
BDD • defined as apreoccupationwithanimagineddefect in one’sappearance. • Alternatively, if a slightphysicalanomalyispresent, theperson’sconcernismarkedlyexcessive. • DSM-IV, thepreoccupationshouldlastfor at leastanhour a day1 and cause clinicallysignificantdistressorimpairment in social, occupationalorotherimportantareas of functioning. • Anxiety and depression has a prevalence of 26.8% to 40% in bddpatients.
Bddassessment • BDDQ (sensitivityof 100 % and a specificity of 89–93 %) • Are youveryworriedaboutyourappearance in anyway? • Doesthisconcernpreoccupyyou? Thatis, do youthinkaboutit a lot and wishyoucouldworryaboutitless? Howmuch time do youspendthinkingaboutit? (more than 1 h per dayissuggestive and more than 3 hrishighlyspecificfor BDD). • Whateffect has thispreoccupationhadonyourlife? • Has it: Significantlyinterferedwithyour social life, schoolwork, job, otheractivities, orotheraspects of yourlife? Causedyou a lot of distress? Affectedyourfamilyorfriends?
BDD assessment • DysmorphicConcernQuestionnaire(DCQ) 7 items. • Yale Brown ObsessiveCompulsiveScale
Conclusion • Complete surgical plan need to be documentedbeforesurgery. • Patientselectionshouldnotonlyhave a preoperatoryassessmentpurelyfromtherhinologicalstandpoint; psychologicalaspectsshould be considered as well. • Standarization of Assessment.