Download
1 / 1
10 likes | 116 Views
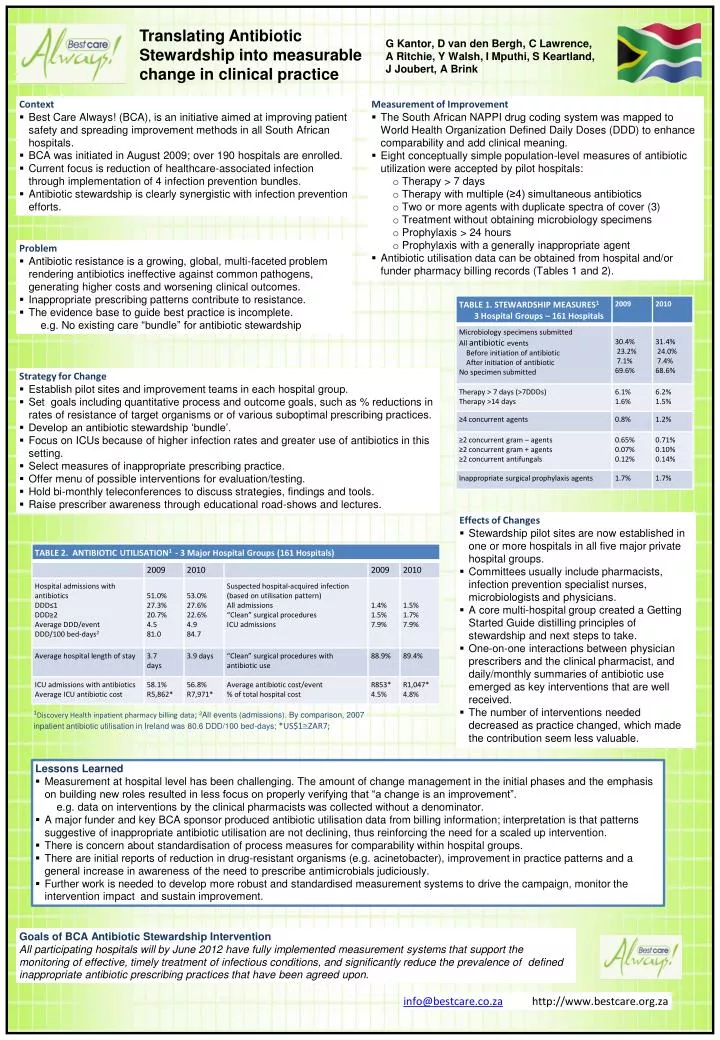
Translating Antibiotic Stewardship into measurable change in clinical practice. G Kantor, D van den Bergh, C Lawrence, A Ritchie, Y Walsh, I Mputhi , S Keartland, J Joubert, A Brink. Context

E N D
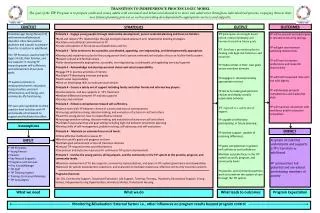
Translating Antibiotic Stewardship into measurable change in clinical practice G Kantor, D van den Bergh, C Lawrence, A Ritchie, Y Walsh, I Mputhi, S Keartland, J Joubert, A Brink • Context • Best Care Always! (BCA), is an initiative aimed at improving patient safety and spreading improvement methods in all South African hospitals. • BCA was initiated in August 2009; over 190 hospitals are enrolled. • Current focus is reduction of healthcare-associated infection through implementation of 4 infection prevention bundles. • Antibiotic stewardship is clearly synergistic with infection prevention efforts. • Measurement of Improvement • The South African NAPPI drug coding system was mapped to World Health Organization Defined Daily Doses (DDD) to enhance comparability and add clinical meaning. • Eight conceptually simple population-level measures of antibiotic utilization were accepted by pilot hospitals: • Therapy > 7 days • Therapy with multiple (≥4) simultaneous antibiotics • Two or more agents with duplicate spectra of cover (3) • Treatment without obtaining microbiology specimens • Prophylaxis > 24 hours • Prophylaxis with a generally inappropriate agent • Antibiotic utilisation data can be obtained from hospital and/or funder pharmacy billing records (Tables 1 and 2). • Problem • Antibiotic resistance is a growing, global, multi-faceted problem rendering antibiotics ineffective against common pathogens, generating higher costs and worsening clinical outcomes. • Inappropriate prescribing patterns contribute to resistance. • The evidence base to guide best practice is incomplete. • e.g. No existing care “bundle” for antibiotic stewardship • Strategy for Change • Establish pilot sites and improvement teams in each hospital group. • Set goals including quantitative process and outcome goals, such as % reductions in rates of resistance of target organisms or of various suboptimal prescribing practices. • Develop an antibiotic stewardship ‘bundle’. • Focus on ICUs because of higher infection rates and greater use of antibiotics in this setting. • Select measures of inappropriate prescribing practice. • Offer menu of possible interventions for evaluation/testing. • Hold bi-monthly teleconferences to discuss strategies, findings and tools. • Raise prescriber awareness through educational road-shows and lectures. • Effects of Changes • Stewardship pilot sites are now established in one or more hospitals in all five major private hospital groups. • Committees usually include pharmacists, infection prevention specialist nurses, microbiologists and physicians. • A core multi-hospital group created a Getting Started Guide distilling principles of stewardship and next steps to take. • One-on-one interactions between physician prescribers and the clinical pharmacist, and daily/monthly summaries of antibiotic use emerged as key interventions that are well received. • The number of interventions needed decreased as practice changed, which made the contribution seem less valuable. 1Discovery Health inpatient pharmacy billing data; 2All events (admissions). By comparison, 2007 inpatient antibiotic utilisation in Ireland was 80.6 DDD/100 bed-days; *US$1@ZAR7; • Lessons Learned • Measurement at hospital level has been challenging. The amount of change management in the initial phases and the emphasis on building new roles resulted in less focus on properly verifying that “a change is an improvement”. • e.g. data on interventions by the clinical pharmacists was collected without a denominator. • A major funder and key BCA sponsor produced antibiotic utilisation data from billing information; interpretation is that patterns suggestive of inappropriate antibiotic utilisation are not declining, thus reinforcing the need for a scaled up intervention. • There is concern about standardisation of process measures for comparability within hospital groups. • There are initial reports of reduction in drug-resistant organisms (e.g. acinetobacter), improvement in practice patterns and a general increase in awareness of the need to prescribe antimicrobials judiciously. • Further work is needed to develop more robust and standardised measurement systems to drive the campaign, monitor the intervention impact and sustain improvement. Goals of BCA Antibiotic Stewardship Intervention All participating hospitals will by June 2012 have fully implemented measurement systems that support the monitoring of effective, timely treatment of infectious conditions, and significantly reduce the prevalence of defined inappropriate antibiotic prescribing practices that have been agreed upon. info@bestcare.co.za http://www.bestcare.org.za