Download
1 / 30
780 likes | 3.37k Views
Thermoregulation in the Newborn. Audra McCay Prince, MD Assistant Professor of Pediatrics Arkansas Children’s Hospital & UAMS Neonatology. Heat Production. Voluntary muscle activity Involuntary muscle activity ( shivering) Non-shivering Thermogenesis. Brown Fat. Locations

E N D
Thermoregulation in the Newborn Audra McCay Prince, MD Assistant Professor of Pediatrics Arkansas Children’s Hospital & UAMS Neonatology
Heat Production • Voluntary muscle activity • Involuntary muscle activity (shivering) • Non-shivering Thermogenesis
Brown Fat • Locations • Abundance in infancy • Differs morphologically • Differs metabolically • Sympathetic enervation
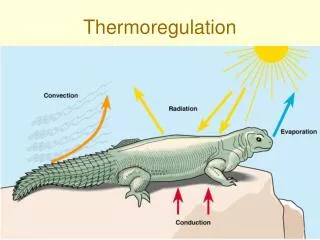
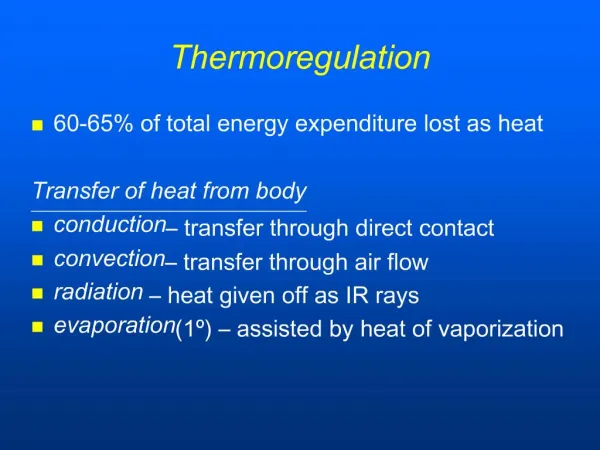
Mechanisms for Heat Loss • Conduction • Convection • Radiation • Evaporation
Conductive Heat Loss • This is heat transfer from a warmer object to a cooler object that it is in contact with. • Example: the baby loosing heat to a cold mattress or scale.
Convective Heat Loss • This is heat transfer from a warmer object to the cooler air. It depends on air flow, as well as the temperature of the air. • Example: the baby on a radiant warmer can have a large amount of convective heat loss, especially in the drafty areas of the nursery.
Radiant Heat Loss • This is heat transfer from a warmer object to a cooler object that are NOT in contact with each other. • Example: heat loss to the walls of the isolette, or heat loss to a cold window next to a crib in the nursery • Transport isolettes
Evaporative Heat Loss • Cooling of the body by the evaporation of water from the skin. • In very small infants this is increased during the first few days of life due to their very thin (non-keratinized) skin, an increased body surface area/body mass ratio, and the extracellular mass is between 80-90% H2O.
Relative Role of Evaporative Heat Loss Kcal/kg/day Birthweight (kg)
Heat Production or O2 Consumption Summit Metabolism Death from Heat Decreasing Body Temp Increasing Body Temp Zone of Thermal Neutrality Environmental Temperature Mernstein G, Blackmon L 1971
Zone of Thermal Neutrality 37 C Body Temperature Inevitable Body Heating Inevitable Body Cooling Thermoregulatory Range Merenstein G, Blackmon L, 1971
Homeotherm • Homeotherms possess mechanisms that enable them to maintain body temperature at a constant level more or less accurately despite changes in the environmental temperature. • An infant that is cooled and not hypoxic attempts to maintain body temperature by increasing the consumption of calories and oxygen to produce additional heat.
Zone of Thermal Neutrality 37 C Body Temperature Inevitable Body Heating Inevitable Body Cooling Thermoregulatory Range Merenstein G, Blackmon L, 1971
Temperature Measurements • Skin temperature • Servo Control • Axillary temperature • Rectal temperature
Specific Situations • In Utero • Delivery Room • Isolette • Radiant Warmer • Open Crib
In Utero • Heat produced in the fetus is dissipated through the placenta to the mother • Fetal temp normally 0.6 0 higher than the mother’s temp • Maternal fever • Epidural anesthesia
Delivery Room • The fetus is born into a cold wet environment, and no longer has the maternal heat reservoir. • When skin is 1st exposed to the air, rapid cooling begins with body temp dropping from 0.2-1.0 c/min. • In response to cold a nor-adrenaline surge occurs. When pursued to an extreme peripheral and pulmonary vasoconstriction occur with sub-sequent decreases in oxygenation and perfusion.
Delivery Room • Careful and immediate drying of the infant’s entire body remains critical in minimizing evaporative heat loss. • Placing on radiant warmer • Hats • Maternal skin
Your Mother was Right Care of the High-Risk Neonate, 4th Edition, Klaus and Fanaroff, 1993, pg 122
Isolette • The importance of double walls • Transport isolettes • Skin temp v. Air temp • Never cover temp probes • Placement of probe is important
Double Walled Isolettes Care of the High-Risk Neonate, 4th Edition, Klaus and Fanaroff, 1993, pg 119
Radiant Warmer • Must use a metallic cover • Air flow is important • Saran wrap • Drapes
Open Crib • Remember that babies continue to have radiant heat loss to the windows, walls, etc., If they are not bundled. • Babies that are losing weight, ex. Feeders and growers may be cold with increased oxygen consumption and caloric expenditure.
Disorders of Temperature Regulation • Hypothermia • Neonatal Cold Injury • Hyperthermia • Asphyxia
Hypothermia • Low birth weight infants • Asphyxia • Prematurity • Sepsis • CNS
Neonatal Cold Injury • LBW • Lethargic and feed poorly • Cold to touch • Red baby • Slow and grunting respirations with bradycardia • edema and sclerema • Metabolic derangements • Pulmonary hemorrhage
Treatment of Cold Injury • Re-warming • Oxygen • Glucose • NaHCO3 • NPO • Antibiotics
Causes of Hyperthermia • Environmental temperature • Infection • Dehydration • Cerebral birth trauma • Drugs
Asphyxia • Resuscitation • Inability to regulate temp • Pay attention to heat loss
Conclusion • Attentiveness to temperature in a sick newborn is extremely important. • Minimizing O2 consumption is the goal. • Recognition and treatment of infants with cold injury can be life saving.