Download

1 / 42
420 likes | 538 Views
Pharmacy Based Needle Exchange. The Can Partnership Claire Raines. Introductions & brief overview of training plan. Who we are Length Break House-keeping Can Partnership Referrals/Open Access. Aims & Objectives.

E N D
Pharmacy Based Needle Exchange The Can Partnership Claire Raines
Introductions & brief overview of training plan • Who we are • Length • Break • House-keeping • Can Partnership • Referrals/Open Access
Aims & Objectives • Promotion of the value of a PBNX to the local community and to the individual. • Enhance awareness of who may use the PBNX • To give insight into why NX exists • To show how you can follow best practice (to run an PBNX with excellence!)
Staff Shoplifting Fear Mistrust Lack Of Confidence Personal Feelings (disgust/distaste) NX Customer Social Embarasment /Stigma Fear Questions/Fear of Low expectations of staff knowledge Feelings / expectations / attitudes
Taking a walk in their shoes exercise • 2 volunteers required!
In their shoes… • Mirrored expectations. • IDUs research shows that heroin users have a more acute ability to spot signs of fear/disgust/anger in a persons facial expressions. • Also that they are very bad at recognising happiness/love/affection. This is thought to be due to expectation of these expressions in family and loved ones. • As a result it’s incredibly important for pharmacy staff to be more aware of their manner when dealing with substance users. • Being more aware of how the transaction may feel for the IDU will also mean they feel less stigmatised, this is also when it is important that the transaction doesn’t happen on the shop floor but in a consultation room.
Staff Respect/polite Positive / friendly Open Confident Confidential / Boundaried Knowledgable PBNX Customer Respectful/Polite Friendly Clear Confidence in staff Open / understanding Knows boundaries Willing to accept advice. Desired expectations / attitudes
Why your pharmacy might offer PBNX ? • You are able to advise on a range of issues including the prevention of drug-related death, overdose prevention, blood-borne infections, oral health, sexual health, contraception and safer sex, nutrition, minor infections, wound dressings, dental health and nicotine replacement therapy. • Opening hours • Alternative option • Location
Why are you providing this service anyway? • You will become one of the ‘gateways’ in bringing people who inject drugs into contact with a range of community services. • To assist the person to remain healthy until they are ready and willing to cease injecting and ultimately achieve recovery . • encouraging people to remain healthy with self-care or to address their other health needs. • To protect health and reduce drug related deaths. • To reduce sharing /risky behaviours by providing sterile injecting equipment, advice and information.
To promote safer injecting practices by providing and reinforcing harm reduction messages - including safe sex advice and advice on overdose prevention (e.g. risks of poly-drug use and alcohol use). • To improve the health of local communities by preventing the spread of blood-borne infections by ensuring the safe disposal of used injecting equipment. • To maximise the access to help of all injectors, especially the socially excluded. • To help people access other health and social care eg: CAN Partnership / The Terrance Higgins Trust/ AA / The Kings Arms Project. • To join close working relationships with other local community services.
& if you’re still not convinced… “The cost of providing health services to someone who injects drugs is estimated to be about £35,000 over their lifetime. The related costs of crime are estimated to be an additional £445,000 over a lifetime.” - NICE.ORG.UK
Why inject? • Substance misuse (Lifestyle,boredom,socialising, experimental,addiction,needle fixation,tolerance levels,coping mechanism,other abuse past or present) • PIEDS (confidence/status,lifestyle,other abuse past or present, self-image/peer pressure/competition/mental health)
Target PBNX population • PBNX’s aim to help people over the age of 18 who inject illicit substances. This includes opioids (eg; heroin) and stimulants (eg; amphetamines or cocaine) either separately or in combination (eg; speed-balling) and also adults who inject non-prescribed anabolic steroids and other performance and image-enhancing drugs (PIEDs).
These customers can include… • High volumes • In a hurry to be served /withdrawing/intoxicated • Sex Workers • Homeless • Dual diagnosis • Clients of services that prescribe • All of the above
1ml RED (A) pack £2.81 • 10 x 1ml combined needle & syringe • 10 x cooking spoons • 10 x citric acid sachets • 10 x alcohol swabs • 1 x 0.25litre bin For I.V use / injecting into surface veins. Suitable for opiate/amphetamine use.
2ml Green (B) pack £2.75 • 10 x 2ml barrel • 10 x Blue 1 ¼” needles • 10 x Green 1 ½”needles* FOR DRAWING UP • 10 x Cooking spoons • 10 x Citric Acid sachets • 10 x Alcohol Swabs • 1 x 0.45litre bin For injecting into deeper veins (femoral/ groin veins). For I.M injecting.
1ml Brown ( C )pack £2.83 • 10 x 1ml combined needle & syringe • 10 x Cooking spoons • 10 x Vit C sachets • 10 x Alcohol swabs • 1 x 0.25litre bin For injecting into surface veins, I.V injecting. Alternative to Red Pack (A) : Vit C instead of Citric Acid
5ml Yellow (D) pack £1.84 • 10 x 5ml barrels • 10 x alcohol swabs • 10 x blue 1¼” needles • 10 x green 1½”needles *FOR DRAWING UP • 1 0.45 litre bin For injecting into deeper veins, I.M injecting. Suitable for steroid injectors.
Pharmacy Needle and Syringe Provision operating policies & procedures might include: • Client dignity, privacy, confidentiality and data protection • Sharps safety • Needle Stick Injury / Body spill proceedure • Individual Syringe Identification • Return of used injecting equipment • Provision for Young People • Client complaints procedure • Signposting
Why do injectors prefer this method? • Different drugs can be introduced into the body in several ways. • Drugs can be snorted, smoked, swallowed, taken rectally, or injected. Each of these processes has the same ultimate purpose – to get the blood into the bloodstream, and to reach the brain!. • Injection has the optimum“Bioavailability” –It is the quickest way and bypasses most barriers to get to the CNS.
What is injected? • Heroin • Amphetamines • Crack • Heroin and crack • Methadone Amps / Sugar Free mixture • Crushed Pills • Steroids • Malanatan/Malanotan 1 and 2 (1=tanning;2=tanning/sexual disfunfunction)stimulates the pigment cells in your body to produce more melanin ,unregulated,from inside out change in skin tone.
Intravenous injection(I.V) • Intravenous injecting is a highly efficient way of introducing drugs into the body. • When drugs are injected - the filtering and delaying mechanisms that protect us when things are absorbed via the gastro-intestinal tract, lungs or skin - are bypassed. • The potential for infection and overdose are increased.
Subcutaneous Injecting(S.C) • Provide handouts • Discuss as a group
Briefly, how do drugs enter and exit our body?. • If drugs are swallowed, the drug is absorbed into the bloodstream through the stomach and the digestive tract. • This process can take a considerable time, an hour or longer. • As mentioned, injecting has the fastest introduction rate of the ways (UTB/Swallowed/Snorted/Oral/Smoked). • Once in the blood stream, the blood from the stomach and the intestines passes through the liver before reaching the heart. • The liver removes toxins from the blood stream, and part of this process includes breaking down substances such as drugs. • Each subsequent pass round the body and through the liver removes more of the drug from circulation.
Arteries & Veins • Arteries take oxygenated blood from the lungs to the rest of the body They branch out, diminishing in size, until they reach the capillaries. • The blood passes through the capillaries in the tissues, releases its oxygen, and is collected again in small veins , which by joining together progressively increase in size. • The arteries return de-oxygenated blood back to the lungs via the heart. All drugs injected into veins must follow a route back through veins of increasing size to the heart. • From the heart the drugs are pumped the short distance to the lungs where the blood passes through the capillaries of the lungs to be re-oxygenated, and then they return to the heart to be pumped to the brain. • (The exception to this description is the pulmonary artery, it carries de-oxygenated blood from the heart to the lungs. All other arteries carry oxygenated blood. The pulmonary vein is unique because it carries oxygenated blood from the lungs to the heart.) • Valves are only found in veins, they assist the flow of blood back to the heart by preventing back flow.
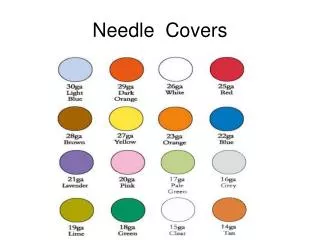
The basic theory behind needle sizes “Needle Gauge” • Needles are measured in terms of their Length, and their Gauge. • Length may be given in millimetres (mm) or in imperial measures. • The size of a needle is also measured by the external diameter of the needle, which is called the Gauge (G or GA). • The hubs of needles are also colour coded, and shorthand for different gauges.This colour-coding only refers to gauge not length.
What happens after injecting? • When a drug is injected into a vein, it reaches the brain via the lungs in a matter of seconds. • The drug is not significantly diluted: hence the experience of the 'rush' or 'hit' as the brain becomes rapidly intoxicated. • The fact that all venous blood must pass through capillaries in the lungs before going to the arteries means that solid matter and air bubbles that are injected into veins cannot reach the brain (except in exceedingly rare circumstances it is only possible if someone has a hole between the chambers of the heart); they will instead get trapped in the capillaries of the lungs.
Intravenous injection • Generally, the arms are the least risky place to access veins for injecting. The main aim of advice given to injectors, (after prevention of spread of blood-borne viruses) should be to maximise the length of time they are able to use the veins in their arms. • When the arm veins can no longer be used, injectors should consider, and workers should promote, switching to a non-injecting route of drug use. • Irreversible damage to the veins can occur where there is: • Repeated use of the same injecting site • Poor technique • Injection with blunt needles • Injection with needles that are too large • Injection of irritant substances.
Injecting Steroids • A large proportion of the products on the market are low-quality fakes, containing little or no active ingredients. • Standards of production are highly variable, and products are liable to be manufactured in non-sterile • environments. • Products are available in oral preparations, single dose ampoules and multi-dose bottles. • Solutions for injection are intended to be injected intramuscularly, and often oil-based,resulting in a thicker solution than water based preparations.
Basic advice that will help to keep veins and skin healthy include: • Wash hands before and after ,clean sites before with a swab, apply pressure after. • Keep personal equipment in a defined, clean area. • Use sterile equipment only, once only, do not reuse • Do not share • Dispose of items safely • Introduce, inject and remove needles gently and slowly at a shallow angle towards the heart. • Alternate injection sites, allowing veins to rest and recover -Smoke rather than injecting at times in order to rest veins • Become ambidextrous so that they can inject in both arms it is best to encourage this before the onset of any problems, as it is much easier to practise new techniques when relaxed and the outcome is not crucial • Discourage use of tourniquets, release them prior to injecting • Stay away from sites that have become infected , get medical help. • Do not flush /back-load/front-load • Do not inject where you feel a pulse or if the blood is bright red. Just how dangerous injecting will be on any one occasion is affected by: The understanding the injector has of their underlying structures The dexterity of the injector The state of mind of the injector (e.g. intoxicated or not) The substance being injected Luck.
Discretion • When handing over the exchange materials, consider using a suitable bag, typically an opaque dispensing bag • This opportunity can be taken for health-promotion activities/leaflets/flyers & advice booklets.
Sharps/ Needle-stick Injuries • Clean it • Report it • Call for help • Get treated • ID source / needle /patient if possible.
Best Practice - Pharmacy-based needle exchange operation Be aware of policies & protocols for : • Young people • The Intoxicated • Psychological instability • Body spills • Staff Hep B vaccinations • Client confidentiality - including what to do when a patient requests needle exchange who is also being prescribed substitute medication. Dealing with unacceptable behaviour / guidance on: – what constitutes unacceptable behaviour – ways of minimising unacceptable behaviour.
Working with Young Service Users Adult models of Needle Exchanges are not appropriate for young people (a person under the age of 18). • It is therefore recommended that Pharmacy Needle Exchanges do not provide this service to those under, or who appear to be under 18 years of age. • The course of action to a young person presenting to a Pharmacy Needle Exchange will be as follows: • Request proof of the young person’s age before making a decision whether or not to provide injecting equipment; • Provide details of specialist local services working with young people with addictions, which will offer advice, information and specialist assessment
Directing under 18’s to Bedford’s Young Person’s Services Plan B Bedfordshire 22 Grove Place, Bedford MK40 3JJ : Tel: 01234 344 911 Plan B offers a range of support, information and advice to young people aged between 5 and 18 who use drugs and/or alcohol and also supports young people affected by someone else’s use.
Further research for the keen. • Safer Injecting http://www.kfx.org.uk/resources/nx08.pdf • Steroids (PIEDS) http://www.siedsinfo.co.uk/ • Guidance with PBNX National Institute for Clinical Excellence Guidelines - www.nice.org.uk. • The Can Partnership Can.org.uk