Download
1 / 65
770 likes | 1.93k Views
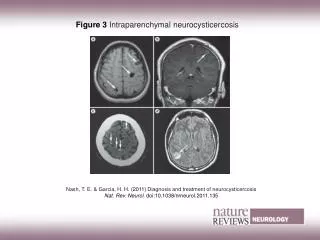
Neurocysticercosis. Mehila Z. March 19 th 2007. Introduction Cysticercosis. Cysticercosis is a systemic illness caused by disseminated larval form of pork tapeworm, Taenia solium . Encystment of larvae can occur in almost any tissue.

E N D
Neurocysticercosis Mehila Z. March 19th 2007
Introduction Cysticercosis • Cysticercosis is a systemic illness caused by disseminated larval form of pork tapeworm, Taenia solium. • Encystment of larvae can occur in almost any tissue. • Involvement of the central nervous system, known as neurocysticercosis (NCC), is the most clinically important manifestation of the disease.
Introduction Neurocysticercosis • Most common helminthic disease of the nervous system. • Common in Latin America, Asia, sub-Saharan Africa, India, and east Asia as well as in industrialized nations with a high immigration rate. • 50 million people worldwide. • In endemic regions, leading cause of hospital admissions and the major cause of acquired epilepsy. • Affect men and women equally. Inflammation around parasites may be more severe in women than in men.
Etiopathogenesis • The adult tapeworm resides in the upper jejunum. • The scolex attaches by both sucking disks and two rows of hooklets. • Often 1 adult worm is present, which may live for years. • usually about 3 m long, as many as 1000 proglottids, each of which produces up to 50,000 eggs. • three to five proglottids are generally excreted into the feces,& the eggs in these proglottids are infective for both humans and animals. • The eggs may survive in the environment for several months.
Kingdom: AnimaliaPhylum: PlatyhelminthesClass: CestodaOrder: CyclophyllideaFamily: TaeniidaeGenus: TaeniaSpecies: T. solium
Etiopathogenesis • Humans = definitive hosts. • Pigs are intermediate hosts • (Taeniasis), without symptoms. • Intermittent fecal shedding. • Embryos penetrate the GI mucosa of the pig (cysticerci). • When undercooked pork is consumed, intestinal tapeworm will again be formed, completing the life cycle • Within 60 to 90 days, the encysted larval stage develops.
Etiopathogenesis • Human cysticercosis occurs when T solium eggs are ingested via fecal-oral transmission from a tapeworm host. • The human then becomes an accidental intermediate host, with development of cysticerci within organs. • Cysticerci may be found in almost any tissue. The most frequently reported locations are skin, skeletal muscle, heart, eye, and most importantly, the CNS (NCC).
Etiopathogenesis • Autoinfection. • Fecal-oral autoinoculation. • Regurgitation of proglottids into the stomach. • Only 5 - 40 % of patients with cysticercosis have an adult worm in their intestine. • Most individuals with intestinal tapeworm infection do not develop symptomatic cysticercosis. • Cysticerci are liquid-filled vesicles consisting of a membranous wall and a nodule containing the invaginated scolex. The scolex has a head armed with suckers and hooks and a rudimentary body.
Stages Of Cysticercosis • Three stages of development. • Vesicular phase, • Parasite is a cyst with thin membrane liquid filled, transparent. • Can remain for decades in this stage. • Or degenerate that ends up with the death of the parasite. • Colloidal-granular stage, • Vesicular liquid becomes viscous and cloudy, • Wall and scolex is transformed granular structure. • No longer is viable. • Nodular calcified stage, • Parasite becomes a calcified.
Vesicular Vesicular-colloidal Granular Calcific colloidal
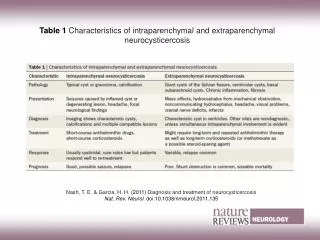
Clinical Features Cysticercosis • Clinical syndromes of cysticercosis. • Neurocysticercosis (NCC). • Parenchymal. • Extra-parenchymal. • Intra-ventricular. • Subarachnoid. • Spinal involvement. • Extra-neural manifestations. • Eye. • Muscle. • Subcutaneous tissue. • Oncospheres actively migrate Vs enter tissues passively during high blood flow.
Diagnostic Criteria (Cysticercosis)Adapted from Del Brutto et al.(Proposed diagnostic criteria for neurocysticercosis. Neurology 2001; 57:177–183) Absolute criteria: • Histological demonstration of the parasite, • cystic lesions showing the scolex on CT or MRI, • direct visualization of ocular parasites by fundoscopic examination Major criteria: • Lesions highly suggestive of neuro-cysticercosis on neuro-imaging, • positive serum enzyme-linked immunoblot for anti-cysticercal antibodies, • resolution of cysts after therapy after anti-parasitic therapy, • spontaneous resolution of small single enhancing lesions Minor criteria: • Lesions compatible with neurocysticercosis on neuroimaging, • clinical manifestations suggestive of neurocysticercosis, • positive CSF ELISA for anti-cysticercal antibodies or cysticercal antigens, • cysticercosis outside the CNS Epidemiologic criteria: • Evidence of a household contact with Taenia solium infection, • individuals coming from or living in an area where cysticercosis is endemic, • history of frequent travel to disease-endemic areas. • Definitive diagnosis: • one absolute criterion or two major plus one minor and one epidemiologic criterion • Probable diagnosis: • one major plus two minor criteria, • one major plus one minor and one epidemiologic criterion, • or three minor plus one epidemiologic criterion.
A 42-year-old man admitted at Nelson Mandela Academic Hospital (Umtata) South Africa presented with a history of recurrent generalized tonic-clonic epileptic seizures of six years duration, disseminated nodules all over the body of two-year duration and headache. • Multiple subcutaneous nodules on the chest wall and a few calcified lesions on chest X-ray
Clinical Features Neurocysticercosis • Many patients are asymptomatic.(80%). • Inflammatory response develops around a degenerating cysticercus. • It is not known what triggers this degeneration. • Peak presentation occur three to five years after infection, but it can be delayed for >30 years. • Sub acute to chronic onset, (except seizures).
Clinical Features • Parenchymal cyst • Calcific cyst • Cysticercal encephalitis • Sub-arachnoid cyst • Racemose cyst • Ventricular cysts • Spinal cyst • Other forms
Clinical Features Parenchymal cysts • 29-62% percent • cerebral cortex or basal ganglia. • usually <1 cm in diameter but can be much larger. • frequently seizures, 50 to 80 percent of patients • The risk of epilepsy in sero-positive individuals is two to three times higher than in sero-negative controls
Clinical Features Parenchymal cysts • The seizures may be focal or generalized • Neurologic examinations are usually normal, • focal neurologic signs may be present. • Severe headaches, rarely fever or signs of meningeal irritation. • Symptoms of increased ICP. • Intellectual deterioration and psychiatric presentations also occur.
Clinical Features Calcific Cysts • Clinically active. Seizures and focal neurologic symptoms • Periodic or episodic peri-lesional edema • May be associated with severe symptoms including seizures and focal neurologic deficits
Clinical Features Cysticercal Encephalitis • Massive cysts in the brain parenchyma, • An intense immune reaction can occur, • Encephalitis and diffuse brain edema. • Fever, headache, and hydrocephalus, with vomiting, impaired consciousness, reduced visual acuity, and seizures. • Spontaneously, or provoked by therapy that causes a large number of cysts to degenerate. • This presentation is most common in children and young females for unknown reasons.
Clinical Features Subarachnoid Cysts • 27-56% • Cysticerci that lodge in the sub-arachnoid space may grow to 10 cm or more since they are not limited by pressure from the brain parenchyma. • Meningeal inflammation and abnormal thickening of the leptomeninges at the base of the brain can result, which can lead to entrapment of the cranial nerves manifest as visual field defects and cranial nerve palsies. • Hydrocephalus can also develop from arachnoiditis and secondary occlusion of the foramen of Luschka or Magendie. • Inflammation can also involve the walls of blood vessels, leading to a proliferative angiitis and vascular obstruction with secondary cerebral infarcts. Focal neurologic motor signs, ataxia, and sensory dysfunction can result, and this presentation tends to be associated with a relatively poor prognosis.
Clinical Features Racemose Cysticercosis • Is characterized by proliferating lobulated cysts without scolices, • Usually found in the ventricular system and sub-arachnoid space. • These cysticerci undergo disproportionate growth of their membrane, with extensions of membranes that group in clusters resembling bunches of grapes. • Infrequent, but the most serious; associated with arachnoiditis, basilar meningitis and hydrocephalus.
Clinical Features Ventricular Cysts • Floating freely or attached to the choroid plexus. • 10 to 20 percent of patients. • Inflammatory responses > granular ependymitis > obstructive hydrocephalus and raised intracranial pressure of gradual or acute. • Associated symptoms; seizures, focal neurologic signs or dementia. • Mobile cysts in the forth ventricle > intermittent obstruction > leading to episodes of sudden loss of consciousness related to head movements (Bruns' syndrome).
Clinical Features Spinal cysticercosis • 1 to 3 percent of cases of NCC. • Intra-medullary or in the sub-arachnoid space. Extra-medullary more common. • Lesions in the thoracic segments are most common. • Inflammatory & demyelinating changes in the peripheral nerve roots. • Patients typically present with radicular pain or paresthesias and may also have sphincter disturbances.
Cysticercosis at other sites • Occular • 1-3% often asymptomatic • Sub-retinal space or vitreous humor • exclude by a proper ophthalmologic examination in all patients with NCC prior to initiating therapy • Inflammation around degenerating cysticerci threatens vision • chorioretinitis, • retinal detachment • vasculitis.
Cysticercosis at other sites • Subcutaneous and intramuscular cysticercosis • almost any body site, • muscle(10%), subcutaneous tissues(75%). • usually asymptomatic, subcutaneous pea-like nodule. • more common in patients from Asia & Africa than from Latin America. • heavy muscle involvement > acute myopathy • SC calcification can be detected incidentally with routine X-rays • Cysts in the heart may be asymptomatic or may result in arrhythmias and/or conduction abnormalities
History Asymptomatic Epilepsy Headache Intracranial HTN Stroke Neuro-psychiatric Hydrocephalus Others Intra-sellar Spinal Ocular systemic Physical examination Cognitive decline Dysarthria Extra-ocular movement palsy or paresis Hemiparesis or hemiplegia, which may be related to stroke, or Todd paralysis Hemi-sensory loss Movement disorders Hyper/hypo-reflexia Gait disturbances Meningeal signs In general
Diagnosis • Extent of work-up depend on clinical presentation. • Incidental finding during unrelated reasons, • Seizures or neurologic symptoms, further investigation. • Routine lab tests • Imaging • Serology • CSF examination • Pathology • Others • Criteria
Diagnosis • Routine lab tests. • Non specific CBC and liver function tests. • Moderate eosinophilia is occasionally present. • Stool examinations eggs are typically not found. • Plain x-ray. • SC nodules. • IC calcification.
Diagnosis • CT/MRI. • Nonspecific, other brain lesions, abscess or malignancies. • Pathognomonic lesion = scolex identified as a mural nodule within the cyst. • MRI preferred over CT. • Sensitive in detecting small lesions, • Brainstem or intra-ventricular lesions, • Better for visualizing the scolex.
Diagnosis • Serology. • Anti-cysticercal antibodies/ cysticercal antigens. • ELISA, crude or partially purified antigens, frequently cross-reacted with other helminthic antibodies. • 75 percent sensitivity. • EITB, (enzyme-linked immunoelectrotransfer blot assay), uses affinity-purified glycoprotein antigens. • Sensitivity and specificity of 100 and 98 percent. • Sensitivity of the EITB falls to <70 % with inactive calcified lesions or a single cerebral lesion. • Serum or CSF, higher sensitivity on serum. • Antibodies can persist for years after the death of parasites,
Diagnosis • Serology. • Antigen testing. • Detect live parasites. • Monitoring patients following therapy. • Parasite antigen levels typically fall by three months after successful treatment.
Diagnosis • CSF examinations. • Helpful. • Raised intracranial pressure. • Normal glucose, mildly elevated protein & white cell. • Sometimes the CSF white cells are predominantly eosinophils. • However, the degree of abnormality in the CSF depends upon whether cysts are adjacent to or have contact with the sub-arachnoid space. • Serologic testing for anti-cysticercal antibodies or parasite antigens can also be performed.
Diagnosis • Pathology. • A single brain lesion with no characteristic scolex. • Negative serology. • Epidemiology. • Cyst location. • Skin or muscle lesion. • The cysticercus will appear as. • A white fluid-filled bladder about 5 to 10 mm in diameter. • Containing a solid 2 mm long larval tapeworm scolex.
Macroscopic Pathology Macroscopic aspect of parenchymatous cysticercus in diverse evolutionary stages: vesicular cysts (straight arrow), colloidal cysts (curved arrow), granulomas (arrow head) and calcifications (open arrow).
Diagnosis Adapted from Del Brutto et al.(Proposed diagnostic criteria for neurocysticercosis. Neurology 2001; 57:177–183) • PCR not yet available. • Diagnostic criteria. • Absolute criteria: • Histological demonstration of the parasite, • Cystic lesions showing the scolex on CT or MRI, • Direct visualization of ocular parasites by fundoscopic examination. • Major criteria: • Lesions highly suggestive of neuro-cysticercosis on neuro-imaging, • Positive serum enzyme-linked immunoblot for anti-cysticercal antibodies, • Resolution of cysts after therapy after anti-parasitic therapy, • Spontaneous resolution of small single enhancing lesions. • Minor criteria: • Lesions compatible with neuro-cysticercosis on neuroimaging, • Clinical manifestations suggestive of neuro-cysticercosis, • Positive CSF ELISA for anti-cysticercal antibodies or cysticercal antigens, • cysticercosis outside the CNS. • Epidemiologic criteria: • Evidence of a household contact with Taenia solium infection, • Individuals coming from or living in an area where cysticercosis is endemic, • History of frequent travel to disease-endemic areas. • Definitive diagnosis: • One absolute criterion or two major plus one minor and one epidemiologic criterion. • Probable diagnosis: • One major plus two minor criteria, • One major plus one minor and one epidemiologic criterion, • Or three minor plus one epidemiologic criterion.
Absolute CriteriaHooks(open arrow) and the spiral canal (small arrows)
Funduscopic visualization of a sub-retinal cystCystic lesions showing the scolex on neuro-imaging
Massive non-encephalitic neurocysticercosis. Cysticercosis Working Group in Peru.
Diagnosis • PCR not yet available. • Diagnostic criteria. • Absolute criteria: • Histological demonstration of the parasite, • Cystic lesions showing the scolex on CT or MRI, • Direct visualization of ocular parasites by fundoscopic examination. • Major criteria: • Lesions highly suggestive of neuro-cysticercosis on neuro-imaging, • Positive serum enzyme-linked immunoblot for anti-cysticercal antibodies, • Resolution of cysts after therapy after anti-parasitic therapy, • Spontaneous resolution of small single enhancing lesions. • Minor criteria: • Lesions compatible with neuro-cysticercosis on neuroimaging, • Clinical manifestations suggestive of neuro-cysticercosis, • Positive CSF ELISA for anti-cysticercal antibodies or cysticercal antigens, • cysticercosis outside the CNS. • Epidemiologic criteria: • Evidence of a household contact with Taenia solium infection, • Individuals coming from or living in an area where cysticercosis is endemic, • History of frequent travel to disease-endemic areas. • Definitive diagnosis: • One absolute criterion or two major plus one minor and one epidemiologic criterion. • Probable diagnosis: • One major plus two minor criteria, • One major plus one minor and one epidemiologic criterion, • Or three minor plus one epidemiologic criterion.
Major Criteria Lesions highly suggestive of NCC on neuro-imaging studies, including: sub-arachnoid racemose cysts (A), enhancing lesions (B), and parenchymal brain calcifications
CT before (left, top and bottom), 1 month (center, top, and bottom), and 3 months after (right, top and bottom) a 1-week course of albendazole. Note the resolution of parenchymal brain cysticerci as the result of therapy.
Contrast-enhanced MRI (A) showing a small single enhancing lesion corresponding to a colloidal cysticercus. Control MRI (B) was taken 16 weeks after showed spontaneous resolution of the lesion.
Diagnosis • PCR not yet available. • Diagnostic criteria. • Absolute criteria: • Histological demonstration of the parasite, • Cystic lesions showing the scolex on CT or MRI, • Direct visualization of ocular parasites by fundoscopic examination. • Major criteria: • Lesions highly suggestive of neuro-cysticercosis on neuro-imaging, • Positive serum enzyme-linked immunoblot for anti-cysticercal antibodies, • Resolution of cysts after therapy after anti-parasitic therapy, • Spontaneous resolution of small single enhancing lesions. • Minor criteria: • Lesions compatible with neuro-cysticercosis on neuroimaging, • Clinical manifestations suggestive of neuro-cysticercosis, • Positive CSF ELISA for anti-cysticercal antibodies or cysticercal antigens, • cysticercosis outside the CNS. • Epidemiologic criteria: • Evidence of a household contact with Taenia solium infection, • Individuals coming from or living in an area where cysticercosis is endemic, • History of frequent travel to disease-endemic areas. • Definitive diagnosis: • One absolute criterion or two major plus one minor and one epidemiologic criterion. • Probable diagnosis: • One major plus two minor criteria, • One major plus one minor and one epidemiologic criterion, • Or three minor plus one epidemiologic criterion.
Minor Criteria • Lesions compatible with NCC on neuro-imaging studies, hydrocephalus (A), and multiple filling defect in the column of contrast material in a myelogram (B)
Treatment • Intestinal T. solium • Praziquantel is first line treatment for all tapeworm infections • 5 to 10 mg/kg in a single dose is administered for taeniasis (T. saginata and T. solium) and diphyllobothriasis; • Efficacy is >95 percent. • Niclosamide an alternative for Taeniasis & other tapeworms. • The recommended dose • Is 4 tablets in a single dose (2 g) for adults, • 2 tablets (1 g) for children 11 to 34 kg, • And 3 tablets (1.5 g) for children >34 kg. • Niclosamide is no longer available in the united states.