Download

1 / 39
400 likes | 675 Views
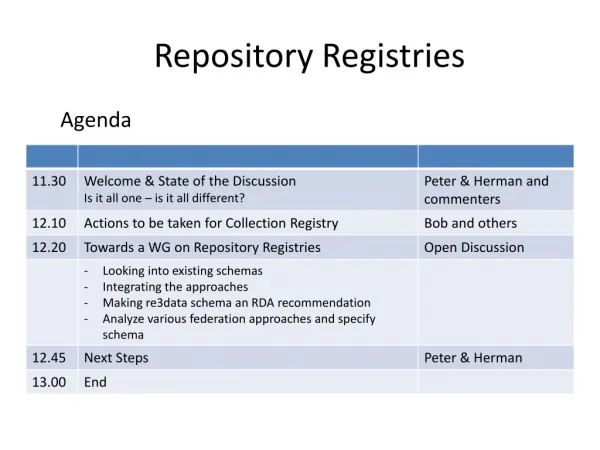
Left Main Stem Intervention Trials & Registries. Keith D. Dawkins MD FRCP FACC Southampton University Hospital UK. Presenter Disclosure Information. The following relationships exist related to this Presentation. Advisory Board or Consultant: Abbott Boston Scientific Corporation

E N D
Left Main Stem InterventionTrials & Registries Keith D. Dawkins MD FRCP FACCSouthampton University Hospital UK
Presenter Disclosure Information The following relationships exist related to this Presentation. Advisory Board or Consultant: Abbott Boston Scientific Corporation ConorMed Eli Lilly Guidant Nycomed
Assessing the Left Main Data • Anatomy: Ostium, Body, Bifurcation • Elective vs. Emergency • Surgical candidate or not? • Left Ventricular Function • Protected or not? • Co-Morbidity: Diabetes, Renal impairment • Technical Approach: Debulking, IVUS, IABP • Drug Elution?
Why is the Left Main special? • Concern over haemodynamic stability • Concern in relation to the consequences of coronary dissection • Unknown comparative efficacy of the available bifurcation techniques • Doubt concerning long-term results
Balloon Angioplasty 1977 Bare metal stents 1993 Drug-Eluting stents 2002
Left Main Stem: Ultima Registry N=279 BMS 68.8%, DES 0%, POBA 15.1% Events (%) Cardiac Death Q-AMI MACE CABG Tan WA. Circ 2001;104:1609-1614
Drug-Elution Bare Metal The contribution of DES to LMS outcomes remains uncertain!
LMS: Medical Treatment + Medical Treatment Left Main Stem Mortality (5 years) = 36.5% Odds Ratio (vs. CABG) = 0.32 [0.15-0.70], p=0.04 Yusuf et al. Lancet 1994;344:563-570
CABG PCI OR
Off/On Pump CCAB Left Main Stem: CABG Mortality N=3904 Death (%) Beauford 12 mths Mack 1m Lu 12 mths Yeatman 24 mths French Registry 12 mths
p<0.0001 p=0.28 Graft PatencyLIMA, SVG and Radial artery grafts Occluded (%)* SVG LIMA Radial *Mean follow-up 565 ± 511 days Khot UN et al. Circ 2004;109:2086-2091
European Revascularisation per million population 7.6% 10.1% 12% Unger F (2004)
p<0.002 Graft Patency: On-Pump vs. Off-Pump Patency Rate (%)* On-Pump Off-Pump *Mean follow-up 3 months Khan NE et al. N Engl J Med 2004;350:21-28
Length of hospital stay, mortality rate, and long-term neurological function and cardiac outcome appear to be similar in the two groups. To definitively answer the remaining questions of whether either strategy is superior, a large-scale prospective randomized trial is required. Circ 2005;111:2858-2864
P C I C A B G Evolution of Revascularization • Off pump technique • Less invasive approach • Increased arterialrevascularization • Optimal perioperative monitoring ? • Improved technique • Improved stent design • DES • Restenosis • Repeat revascularization • High costs • Invasive Over the last decade, the standard of care for both CABG and PCI has continuously improved, leveling the playing field.
SynTax: All-Comers Design PCI all captured w/ follow up CABG 2750 captured (750 w/ follow up) TAXUS CABG vs Run-In Qualification Phase Site Selection All patients with 3VD/LM Heart Team (surgeon & interventionalist) amenable for both treatment options amenable for only one treatment approach Randomized Arm N=1800 (1:1) Two Registry Arms
Run-in Phase Data: Overall Results 8895 12072 Run-in phase data 3177 Total # CABG patients Total # PCI patients Total # patients entered as of 12 May 2005
Run-in Phase Data: Overall Results CABG (103 Sites) 86.4 PCI (104 Sites) 60.3 Mean # of Patients/Site 30.5 26.0 22.3 8.3 Total Patients 3VD Left Main Patient ratio of PCI:CABG is 1:3 Ratio of PCI:CABG for both 3VD and LM disease is 1:3
Run-In Phase: Left Main Data CABG (103 Sites) PCI (104 Sites) 26.0 Mean # of Patients/Site 14.5 7.1 8.3 2.7 1.8 2.6 2.3 1.9 1.5 Mean Isolated +1VD +2VD +3VD PCI:CABG ratio for LM+3VD is 1:10
Run-In Phase: Left Main Data Europe North America 31.3 24.2 20.6 Mean # of Patients/Site 12.4 8.1 6.7 8.4 7.9 2.9 2.1 1.8 0.8 3.8 2.2 2.4 2.0 1.8 2.0 1.4 0.7 Mean Isolated Mean Isolated +1VD +2VD +3VD +1VD +2VD +3VD CABG: Total LM - 1867 CABG: Total LM - 813 PCI: Total LM - 648 PCI: Total LM - 212 Similar rates & types of LM procedures were performed in Europe & North America.
Run-In Phase: Left Main PCI Data Europe (77 sites) North America (27 sites) 8.4 7.9 Mean # of Patients/Site 5.6 1.8 Total LM Unprotected Unprotected LM PCI procedures were performed 3X more often in Europe than in North America.
Left Main Disease Procedures Mean number of patients per site The Netherlands performs twice the number of LM PCI, while Belgium performs half, versus the rest of Europe
Left Main PCI Procedures Average number of LM patients with PCI per site The majority of LM PCI procedures in The Netherlands are unprotected.
Left Main PCI Procedures Average number of LM patients with PCI per site Almost half of Netherlands LM procedures are isolated LMs; approx. 1/3 of all LM in Germany are LM+3VD
445 416 282 163 37 SynTax Enrollment Oct 14th 2005
Randomized Data + DES Left Main None!
DES + LMS Registries *19 protected LM Park S-J. J Am Coll Cardiol 2005;45:351-356 Valgimigli M. Circ 2005;111:1383-1389 Chieffo. Circ 2005;111:791-795
DES Registries: Bifurcation treatment • Single stent • Kissing stents • Culotte • Crush stents • V stents • T stents • Reverse crush ± Final Kissing balloons
Left Main: Major Adverse Cardiac Events MACE Free (%) FU 12 months FU 6 months FU 17 months Park S-J. J Am Coll Cardiol 2005;45:351-356 Valgimigli M. Circ 2005;111:1383-1389 Chieffo. Circ 2005;111:791-795
Left Main: Death Death (%) FU 12 months FU 6 months FU 17 months Park S-J. J Am Coll Cardiol 2005;45:351-356 Valgimigli M. Circ 2005;111:1383-1389 Chieffo. Circ 2005;111:791-795
DES Better BMS Better 6 5 4 3 2 1 0 1 2 3 4 Multivariate Predictors Distal Left Main Disease DES Use LVEF % Parsonnet Score Reference Vessel Diameter Shock Presentation Troponin T >0.02 µg/l Valgimigli M. Circ 2005;111:1383-1389
DES Better BMS Better 6 5 4 3 2 1 0 1 2 3 4 Multivariate Predictors Distal Left Main Disease DES Use LVEF % Parsonnet Score Reference Vessel Diameter Shock Presentation Troponin T >0.02 µg/l Valgimigli M. Circ 2005;111:1383-1389
Conclusions • Randomized trials (DES vs. CABG) are required. • They are unlikely to be powered for lesion sub-sets because of variations in PCI approach. • In planning Left Main PCI, consider individual patient and lesion specific risk factors. • Plan the strategy…