Download
1 / 21
210 likes | 362 Views
VULNERABLE PLAQUES: Pertinent d oubts and solutions in interventional cardiology. EuroPCR Paris, 16 May 2006. Case 1. ♂ 62 year-old CV risk factors: Diabetes mellitus type 2 Hypercholesterolemia. Previous history: NQWMI (1990) > Stenting of prox-RCA

E N D
VULNERABLE PLAQUES:Pertinent doubts and solutions in interventional cardiology EuroPCR Paris, 16 May 2006
Case 1 • ♂ 62 year-old • CV risk factors: Diabetes mellitus type 2 • Hypercholesterolemia • Previous history: NQWMI (1990) > Stenting of prox-RCA • NQWMI (2005) > Stenting of prox-LAD • Actual symptoms: • after an orthopedic operation to the right knee (april 2006), 2 episodes of unstable angina at rest lasting 15’each, with pain referred as the same of the previous NQWMIs without ECG changes but minimal troponine increase • Strategy: Coronary angiogram was planned
Case 1 • Coronary angiogram: • RCA: • Good result of the stent in the proximal part. • No further severe stenoses. • LCA: • Good result of the stent in the proximal part. • 90% stenosis of ostial D1 (covered by the stent in LAD) with TIMI 3 flow, same as just after stenting. • No further severe stenoses.
Case 1 • After Ventriculography (normal LV function with mild inferior hypokinesia): • New onset retrosternal pain, referred as the same as the 2 previous episodes of unstable angina. • New control coronary angiogram: • RCA: same as before. • LCA:…
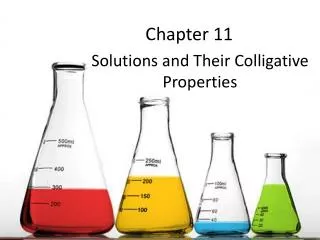
Pre Post
Thrombus in mid-LAD thrombus Non “flow-limiting” thrombus, just at the ostium of a small septal branch, superimposed on an eccentric plaque in the anterior descendens artery plaque
What to do? Pain started increasing again > We decided to stent the lesion The patient could not receive aggressive antithrombotic therapy because of knee hemoarthros after recent surgery. No Abciximab was given, only aspirin and clopidogrel.
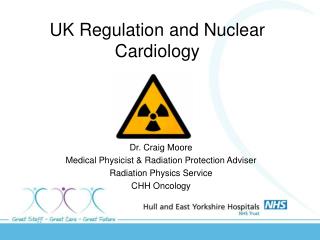
In hospital follow up • Residual pain (not improved after stenting) for 3 hours • (total occlusion of the small septal branch after stenting) Baseline Septal branch After stenting Thrombus • Increase in post-procedural myocardial enzymes (18 h): • CK: 124 U/l (normal: 57-374 U/l) • CK-MB: 21 U/l (normal <16 U/l) • Troponine I: 4.78 ng/ml (normal < 0.08 ng/ml)
Case 2 • ♂ 51 year-old • CV risk factors: Arterial hypertension • No previous cardiac hystory • Actual symptoms: • March 2006:aborted sudden death with VF and out-of- hosptial resuscitation, due to NQWMI • Strategy: Stabilization of the neurological situation • Coronary angiogram planned 15 days after the acute event
Case 2 • Coronary angiogram: • RCA: • Non-dominant small vessel without evidence of severe stenoses. • LCA:…
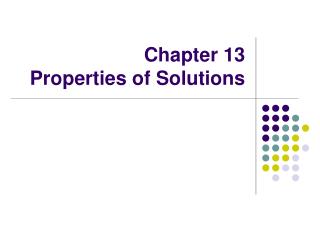
IVUS of mid-LAD Ulcus
Virtual Hystology Non “flow-limiting” ulcerated plaque Predominantly fibrous plaque (stable?)
What to do? Due to the “stable” clinical situation (no cardiac symptoms for 15 days), the “non-flow-limiting” appearance of the lesion at angiography and IVUS, and the “stable” nature of the residual plaque… We treated the patient in a conservative way (aspirin, clopidogrel, statins, B-blockers)
Discussion • Non flow-limiting lesions: • “evolving” situation: thrombus formation superimposed on a potentially thrombus-prone “active” plaque • Versus • “stable” situation: an ulcus in which the vulnerable part of the plaque (the necrotic core) has already disappeared
Discussion • Role of the concomitant pharmacological therapy: • is an aggressive antithrombotic therapy enough to limit thrombus formation and to avoid a complete occlusion of a major epicardial vessel? • what happens if the patient has contraindications to this type of aggressive therapy? • Role of the percutaneous treatment of the lesion: • - is stenting justifed, exposing the patient to the risk of restenosis and stent thrombosis?
For further slides on these topics please feel free to visit the metcardio.org website:http://www.metcardio.org/slides.html