Download
1 / 38
420 likes | 775 Views
INTENTIONAL THALLIUM POISONING – VERIFICATION AND TREATMENT. Pelclová D (1), Šenholdová Z (1), Lukáš E (1), Urban P (2), Lacina L (3), Vlček K (1), Fenclová Z (1), Kitzlerová, E (4). 1. Department of Occupational Medicine, Charles University, Prague

E N D
INTENTIONAL THALLIUM POISONING – VERIFICATION AND TREATMENT Pelclová D (1), Šenholdová Z (1), Lukáš E (1), Urban P (2), Lacina L (3), Vlček K (1), Fenclová Z (1), Kitzlerová, E (4). 1. Department of Occupational Medicine, Charles University, Prague 2. National Institute of Public Health, Prague 3. Department of Dermatology; 4. Psychiatric Department, General University Hospital and First Medical faculty, Charles University, Prague, Czech Republic
THALLIUM • discovered in 1861 by Sir Williams Crooks • 1862 by French chemist Claude-Auguste Lamy • In Greek, thallos "green twig." • Using spectroscopy, the brightest lines in the spectrum of thallium are green • melting point 300º C (576º F) • boiling point 1480º C (2,655º F) • elementary thallium non-toxic • monovalent and threevalent salts very toxic • LD about 900 mg
THALLIUM • rather uncommon element • world production 12tons/year semiconductors, photocells, optic glass, thermometers • in medicine – Tl201radioactive tracer in heart scintigraphy to detect myocardial ischaemia • occurrence in minerals • emissions 1500 tons/year granite, coal
THALLIUM – IN THE PAST • Tl2SO4 has long been used as rodenticide, insecticide • Colorless and tasteless • Tl acetate : treatment of • veneric diseases,ringworm • Depilatory agent • Low therapeutic index • Banned in the 1970ies in most countries
Toxicokinetics – inorganic salts • absorption by all ways, oral about 90% • distribution to all tissues • greatest concentration in the intestines, liver, kidney, heart, brain and muscles • excretion by faeces and urine, • the proportion 2:1 • enterohepatic circulation • half-lives 1-30 days
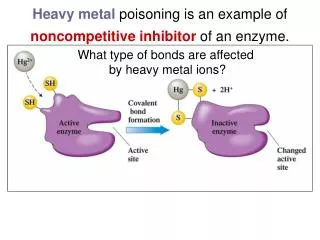
Pathophysiology - 1 • Similarities in charge and ionic radius between K+ and Tl+ ions), Tl substitutes for K: • 1. blocks energyutilizationbyNa-K-ATPasechannel = (active transport of monovalent ions - K+ across cell membrane) Thallium disturbs maintaining of a resting potential across the membrane of active cells - Tl has 10-fold greater affinity. Neuronal, cardiac and skeletal muscle cells • 2. blocks energyproduction from glucose: ADP to ATP by pyruvate kinase = K requiring enzyme - links anaerobic glycolysis to the Krebs cycle) inhibition by binding with 50-fold affinity comparing to K.
Pathophysiology - 2 • 3. damages riboflavin, precursor of FAD forming an insoluble complex and intracellular sequestration of vit. B6 decrease of riboflavin disrupts metabolism by reducing activity of Krebs cycle • 4. binds to SH groups and interferes with formation of disulphide bonds in keratin - structural damage to hair, nails • 5. causes activation or inhibition of other enzymes (ALA synthetase, B12 metabolism…)
2 Case reports • 2 patients, mother and daughter, living in the same household • Very probably intentional poisoning by one member of the family • Oral intake • Chronic
Patient Amother • 44years old • PH: no serious disease • OH: super-market manager • 1. poisoning • November 2004 sudden strong chest pain, following 3 days severe pain with paresthesias in both lower limbs • Symptoms disappeared within 3 weeks, following 3 weeks persisted mild paresthesias and discomfort in the lower limbs
2. poisoning • In March 2005 she developed suddenly a strong muscular pain in the lower limbs. The gait was painful „as on a broken glass“. • within 5 days she became bald. • In April – one month stayed at neurology dept. With suspicion on LI syndrome and posttraumatic stress disorder (anxious, depressive, had work overload and home conflict environment) • EMG, evoked potentials, MRI normal • In June improvement, returned to work
3. poisoning • August 2005 • Progressive pain in lower limbs with paresthesias • Blurred vision – she could differentiate only dark and light spots in the periphery of the visual field • After 3 weeks her condition improved a little • Mild pain in the feet and knees persisted several weeks • Vision difficulties persisted • Eye fundus : n. opticus atrophy
HospitalizationDept. Occupat. Medicine • Admitted on January 31,2006 • 5 months after last intoxication • 1) attempt to prove the poisoning • 2) attempt to improve vision damage – she still could not read EMG: mild motor and sensoric damage, EEG borderline Visual evoked potentials: severe damage with visus • BIOLOGICAL HALF-LIFE of thallium • broad range of 1-30 daysHoffman RS. Toxicol Rev 2003
Patient B: Historydaughter • 22years old woman • PH: no serious disease • OH: high school,1 year maternity leave • FH: mothertreated for symptoms of unknown etiology, father probably psychopathic personality, no treatment, daughter 1 year old, healthy
1 poisoning • In December 2005 suddenly strong pain in lower limbs, maximum in the stockings distribution, ache in the skin of lower extremities • Anorexia • 3rd week symptoms deteriorated, treated with analgesics (tramadol) • 4th week lost all body hair (except eyebrow and eyelashes) • She developed blurred vision, weakness of lower limbs, unable to walk • Hospitalized at neurology dept.
Hospitalization at Neurology Dept. • Blood and urine sent to toxicology screening (drugs, metals incl. Cd, Pb, Hg, Se, Zn, Tl,) • 5th week: vision damage with maximum in the central area, right and left eye • Shortly also speaking difficulties and feeling of heavy tongue • Positive results for thallium in blood and urine
Hospitalization atDept. Occup. Medicine • Admitted on January 26, 2006 • 7th week of symptoms • On admission: • On a wheel chair, paraparesis, motor weakness • Bald (only eyebrow and lashes left) • Could distinguished fingers from 30 cm complained of strong pain in lower limbs • Altered mental status, depressive, anxious • Slow speech, low voice
Antidote • Prussian blue - Fe4[Fe(CN)6]3 (ferric hexacyanoferrate), • Radiogardase, Heyl • CAS 14038-43-8 • discovered 1704 by a Berlin color maker Diesbach • since the 1960s used to treat Cs and Tl poisonings • Binds thallium by ion exchange, adsorption and mechanical trapping within the crystal structure
Specific treatment • Insoluble, low absorption from the GIT (?) • stops enterohepatic circulation of thallium • Increases elimination both to faeces and urine • Advantage: rare side effects, bluish sweat and tears • Reduces half-life from 8 to 3 days • First dose after arrival 6g /12 hours • Continued with 12 g/day in 4 doses
Supportive therapy • 10% mannitol as cathartic • Charcoal (Carbosorb) 2x 25 g/day • Analgesics • Vit. B12, B6 • Topical dermatological treatment supporting hair growth
Thallium concentration in urine µg/lin the daughterTotal excretion 8.4 mg in 32 days, further Tl in faecesAntidotal treatment 22 days
Toxicological analysis in daughter • Thallium found in all biological materials – blood, urine, faeces, hair
Examinations • Neurological (incl. needle EMG, VEP, BAEP, EEG,MRI of the brain) • Ophthalmological (visus, fundus, perimeter) • Dermatological • Further: • ECG, psychiatric,blood biochemical analysis, urinalysis, kidney functions
January 20052nd month • Unable to walk • Severe polyneuropathy • Verified by needle EMG • sensory, motoric and autonomic • Symmetrical • Low extremities only
April 20065th month • Able to walk with a walker leg support. • Severe motor polyneuropatie. Mild improvement, esp. Sensitive and autonomic nerves. • MRI of the brain:normal finding incl. optic nerves, tracts, chiasma and visual cortex • Atrophy of both optic nerves on the ocular fundus
August 20069th month • Still severe motor polyneuropathy • She could walk without support • Unstable gait • Pathology in EEG, VEP, BAEP • Vision of fingers from 0.75 m
Slightly abnormal entrance findings Control: slow improvement 2nd month: no response due to severe vision damage 5th month: Low peak at right side, no response left side. 9th month: Bilaterally abnormal finding low reproducibility and low VEP, worse left side EEG, BAEP VEP
FURTHER FINDINGS • ECG – non-specific ST segment and T wave changes during a febrile state with tachycardia • Transthoracic echocardiography – diffuse hypokinesis of the left ventricle, markers normal • Psychiatric examination • Neuropsychological testing not possible – visual problems • USG of the abdomen normal • Kidney functions normal
Total alopeciadaughter • Reversible • Highest value 36.1 μg/g (5thweek) • Sequential analysis of 1.5 cm hair segments = 6 months • Thallium 5.61- 6.24 – 7.41 – 7.81 – 6.67 μg/g hair • New hair 6thweek of poisoning and 8thday of antidote treatment– drop to 1.6 μg/g)Daniel J Am Acad Dermatol 2004
Trichological analysis of the acute hair loss of the daughter Normal hair • Light microscopy - • The proximal end hair fibre tapered and distorted. • Rough surface of the proximal end • Amorphous cuticular and cortical cells as a sign of the pathological keratinisation. (Metter and Vock 1984)
Trichological analysis of the acute hair loss of the daughter • Under transmitted-light microscopy the cortex dark discolorisation and disorganized on the widened club-shaped end. • Gaseous inclusions under the phase contrast microscopy.
Trichological analysis of the new hair of the mother • Hair of the acute loss not available • Recent hair – normal finding, smooth surface of keratinocytes
Thallium in urine (μg/l)Optical Emission Spectrometer - Inductively Coupled Plasma (OES-ICP)
Thallium in blood and faecesOptical Emission Spectrometer - Inductively Coupled Plasma (OES-ICP)
CONCLUSION - mother • Treatment with Prussian blue produced a higher excretion of thallium in urine • And a measurable amount in faeces • In mother the clinical effect was negligible – • 1¼ year after last poisoning: • EMG: Residual mild axonal sensory neuropathy, mild improvement after 6 months. Autonomic fibers without damage. • Opthalmologic examination: scotomas of upper and central parts of both visual fields • Visual evoked potentials: prologed latency, lower amplitude
CONCLUSION - daughter • 1 year after intoxication • EMG examination - Severe damage in motor and sensory fibers, autonomic normalized already • Ophthalmologic examination – mild improvement • right eye - scotomas in central and medium periphery • left eye – scotomas in central area
SUMMARY • Thallium typically causes damage of peripheral nerves of lower extremities, vision and hair. • Combination of these symptoms suggests thallium poisoning • Late treatment has low effect • Prognosis of hair loss is good • Polyneuropathy improves within months till years • Vision damage has the worst prognosis
THANK YOU • 3rd victim – dog of the family