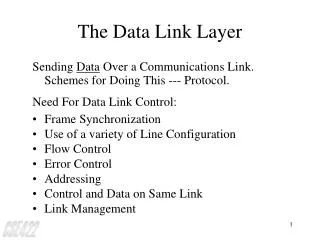
Download
1 / 30
300 likes | 445 Views
Assessment of dietary supplement safety: What can we learn from poison control center data? . Suzanne Hendrich, PhD University Professor, Food Science and Human Nutrition, Iowa State University, Ames, IA 50011 shendric@iastate.edu. Outline.

E N D
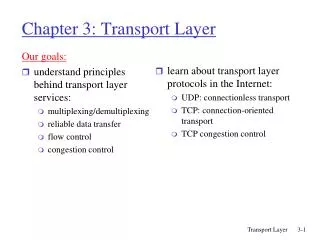
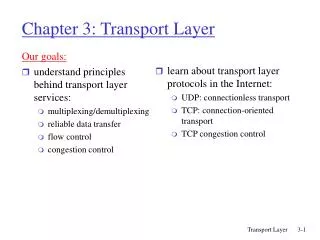
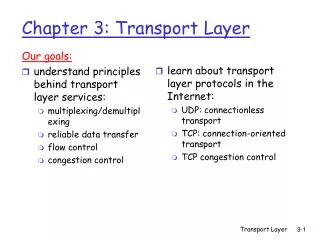
Assessment of dietary supplement safety: What can we learn from poison control center data? Suzanne Hendrich, PhD University Professor, Food Science and Human Nutrition, Iowa State University, Ames, IA 50011 shendric@iastate.edu
Outline • Review of American Association of Poison Control Centers (AAPCC) annual reports • What/how • Summary of AAPCC adverse event data 2003-2012 • Vitamins • Minerals • Dietary botanicals • Implications for consumers and for the food & supplement industries
American Association of Poison Control Centers (AAPCC) • 57 Poison Control Centers, 1-800-222-1222 • AAPCC’s mission is to advance poison centers in their public health mission. • Produces annual data reports for public use • https://aapcc.s3.amazonaws.com/pdfs/annual_reports/2012_NPDS_Annual_Report.pdf • Reports published in Clinical Toxicology • PCs typically directed by Pharm D or RN with board certification in applied toxicology • PC calls handled by health professionals with specific toxicology training
Report data • “…reflects only those cases that are not duplicates and classified by the regional PC as CLOSED. A case is closed when the PC has determined that no further follow-up/recommendations are required or no further information is available. Exposure cases are followed to obtain the most precise medical outcome possible.” AAPCC Ann Rep 2009 • Fatality review team determines if a death should be listed as contributed to by the substance in question.
Substance Categories Most Frequently Involved in Human Exposures (Top 25) AAPCC Ann Rep 2012 Substance (Major Generic Category)All substances%Single-substance exposures% Analgesics 311,347 11.59 202,996 9.99 Cosmetics/Personal Care Products 211,314 7.87 204,110 10.04 Cleaning Substances (Household) 193,802 7.21 172,905 8.51 Sedative/Hypnotics/Antipsychotics 162,634 6.05 62,271 3.06 Foreign Bodies/Toys/Miscellaneous 110,070 4.10 107,067 5.27 Antidepressants 108,773 4.05 45,371 2.23 Cardiovascular Drugs 103,922 3.87 50,012 2.46 Antihistamines 96,997 3.61 69,241 3.41 Topical Preparations 96,431 3.59 94,276 4.64 Pesticides 88,694 3.30 82,916 4.08 Alcohols 74,858 2.79 26,964 1.33 Vitamins 68,168 2.54 59,028 2.90 Cold and Cough Preparations 68,144 2.54 49,547 2.44 Bites and Envenomations 64,787 2.41 63,993 3.15 Antimicrobials 62,426 2.32 51,750 2.55 Stimulants and Street Drugs 61,185 2.28 36,027 1.77 Hormones and Hormone Antagonists 59,449 2.21 40,874 2.01 Anticonvulsants 51,015 1.90 21,757 1.07 Plants 49,374 1.84 46,775 2.30 Gastrointestinal Preparations 49,035 1.83 37,626 1.85 Chemicals 39,571 1.47 33,784 1.66 Dietary Supplements/Herbals 37,729 1.40 30,316 1.49 Hydrocarbons 36,356 1.35 34,178 1.68 Fumes/Gases/Vapors 32,258 1.20 29,338 1.44 Electrolytes and Minerals 31,937 1.19 26,287 1.29
Substances with greatest rate of exposure increase in 2012, AAPCC report • Vitamins were 5th on the list of top 25 substances with increasing rate of exposure, with an increase of 1849 cases over the previous year • Dietary botanical supplements were 13th on the list with an increase of 1215 exposure cases in 2012 compared with 2011
Deaths contributed to by vitamins, minerals and botanical supplements, 2003-2012 (AAPCC annual reports) *2005 Codex Guidelines adopted for vitamin and mineral supplements. #FDA ban on Ephedra upheld by US Appeals Court.
Vitamin exposures reported to PCs • 2006—AAPCC reporting format changes—total single case exposures
Vitamins: major adverse events In July of 2005, Codex Alimentarius Commission adopted the Guidelines for Vitamin and Mineral Food Supplements. (from FDA website)
Vitamin supplements--summary • Exposure reports seem to be fairly constant, with a trend to decrease over the last 4 years. Associated with decreasing exposure reports in children ≤ 5 years of age. • Deaths and major adverse events (requiring hospitalization) are minimal, perhaps benefitted by Codex Guidelines.
Mineral exposures (2003-2012) Note Change in reporting format from 2006-present to show single exposures only.
Major adverse events—mineral supplements—AAPCC reports In July of 2005, Codex Alimentarius Commission adopted the Guidelines for Vitamin and Mineral Food Supplements. (from FDA website)
Deaths contributed to by mineral supplements—AAPCC reports *One death from a multi-botanical/multi-mineral supplement
Mineral supplements--summary • Exposure reports seem to show a slight downward trend since 2008, due to decreasing exposure reports in children ≤ 5 years of age. • Codex guidelines may have helped reduce serious adverse events from 2006 on, especially from Ca, Fe and K, the major contributors before.
Note greater proportion of adult: child exposures compared with vitamins or minerals: but recent trends are that for all three classes (vitamins, minerals, dietary supplements), exposures of young children predominate!
Dietary supplements: major adverse events reported to PCs—2001-2010 FDA published “A Dietary Supplement Labeling Guide” in 2005.
Deaths contributed to by dietary supplements reported to PCs *FDA ban on Ephedra upheld by US Appeals Court. FDA published “A Dietary Supplement Labeling Guide” in 2005. #In 2012, the other death was from a homeopathic supplement.
Trends for dietary supplements • An abrupt change of increased apparent safety after 2005 is noted—related to FDA guidance re: supplement labeling? • Exposures reported especially for children continue to increase—why? • Major adverse events have continued an increasing trend since a low point in 2009. Complex botanical mixtures account for about 1/3 of these; the addition of energy drinks to this category accounts for ~15% of the cases.
Echinacea Ginkgo Garlic Soy Ginger Ginseng Peppermint Fish oil St. John’s wort Glucosamine
Fish oil Glucos- amine Echi- nacea Flaxseed Ginseng Ginkgo Garlic Combi- Herbs Chon- droitin Co-Q-10
Comparing vitamins, minerals and dietary supplements: PC exposure reports 2003-2012
Major adverse effects of vitamins, minerals and botanical supplements: PC reports 2003-2012 Vitamin exposures occur in much greater numbers but with similar numbers of adverse effects compared with minerals. Why the steeper drop in adverse events from dietary supplements? Perhaps credit goes to labeling, regulation, and to scientific findings, but ingredient combinations in dietary supplements may be much more of an issue than with vitamins and minerals; recently increasing adverse events with dietary supplements (including energy drinks) bear this out.
Conclusions • These data suggest that the dietary supplement industry is responsive to government action (Codex, FDA, the Ma huang/ephedra ban worked!) • Nothing could be worse for product sales than serious adverse events and deaths—it is in the industry’s best interests to prevent. • What more needs to be done? • Fe, niacin seem to continue to stand out as posing risks. • Most adverse events with dietary supplements come from mixtures, emerging and unknown products—increased consumer education seems warranted.
Another perspective: comparison of dietary supplement toxicity reports with other foodborne toxicants in AAPCC data • In addition to vitamins, minerals and dietary supplements, AAPCC tracks • Seafood toxins • Plant toxins • Other foodborne toxicants • How do all of these classes of food components compare?
Plant toxins—adverse effects from AAPCC reports (major illnesses) *1 death, the only one reported from 2007-2012 for these major plant toxins.
AAPCC data on food-related toxicities: major adverse events, 2007-12
Comparing food-related toxicities 2007-2012, AAPCC data • Overall, food-associated components pose only minor risks (0-~50 cases/yr in the US), with a relatively constant number of cases over recent history. • Adoption of industry standards may be continuing to mitigate adverse events from vitamins, minerals and dietary supplements. • Complex formulations of some dietary supplements may be contributing to recent modest increases in adverse effects from this diverse class of substances. • Local government and seafood industry surveillance probably contribute to low incidence of toxic effects for these foods. • The advice “buyer beware”, know what you are ingesting insofar as possible remains an appropriate caution.