Download
1 / 18
180 likes | 288 Views
Lessons from the “Canadanish” experience. Lieven Annemans. Universiteit Gent, VUB. Content. Recommendations for improved health (care) policy (VGR) Similarities and differences with Can/Den Towards a blueprint for a Flemish health system Objections against decentralization Final thoughts.

E N D
Lessons from the “Canadanish” experience Lieven Annemans Universiteit Gent, VUB
Content • Recommendations for improved health (care) policy (VGR) • Similarities and differences with Can/Den • Towards a blueprint for a Flemish health system • Objections against decentralization • Final thoughts
Recommendations for health (care) policy • Setting health objectives • According to population needs • Increase focus on prevention • Revise the way health care providers are paid: mix of payment • per practice, per patient, per service, for quality • Improve cost-effectiveness of interventions in health • Better alignment (between prevention and cure; between health and social services, between health and socio-economic status,...) • Adapt education of health care providers to societal challenges VGR , 2006
Recommendations for health (care) policy • Setting health objectives • According to population needs • Increase focus on prevention • Revise the way health care providers are paid: mix of payment • per practice, per patient, per service, for quality • Improve cost-effectiveness of interventions in health • Better alignment (between prevention and cure; between health and social services, between health and socio-economic status,...) • Adapt education of health care providers to societal challenges VGR , 2006
why further decentralization? • More efficient health objectives (also including cure and care) • Payment in function of quality and meeting objectives • Alignment • Between health and social services • Between prevention and cure • Between health and education, work and housing (determinants of health) • Between health and training of health professionals • Better guarantees for integrated care • Avoid blaming, cost shifting, overlap, contradictions, inefficiency, double use, gaps, .... existing in current “semi-decentralized” situation VGR , 2006
Content • Recommendations for improved health (care) policy (VGR) • Similarities and differences with Can/Den • Towards a blueprint for a Flemish health system • Objections against decentralization • Final thoughts
Similarities and differences with Can/Den • Similarities • Federal state - regions - subregions • (Socio)economic differences between regions (Can) • Language issue (Can) • Health insurers (Can) • Differences • Only “decidecentralized” • Cultural differences stronger (cfr J. De Maeseneer) • Bismarck system (social insurance) • Brussels
Content • Recommendations for improved health (care) policy (VGR) • Similarities and differences with Can/Den • Towards a blueprint for a Flemish health system • Objections against decentralization • Final thoughts
Towards a blueprint for a Flemish health system • Financial and political accountability • Spending power • Full responsibility for programming, norms and quality • Integration of prevention, cure and care, and of first, second and third line (double integration) • Alignment with social services and other determinants of health • Central role of the general practioner as gatekeeper (cfr WHO) • Three-layer health care system • Maintaining solidarity, at least for a well defined and agreed period of time • Maintain some functions at the central level (HTA, information system) • Respecting values of equity, effectiveness and cost-effectiveness
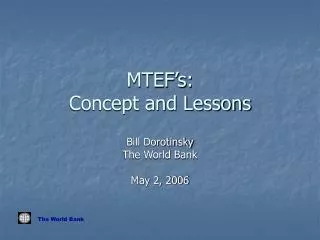
Integrated P C R C A E U R V R E E E N T Promote health Caring for patients W. De Meester, 2005 Cfr RHA’s, cfr LHIN in Ontario
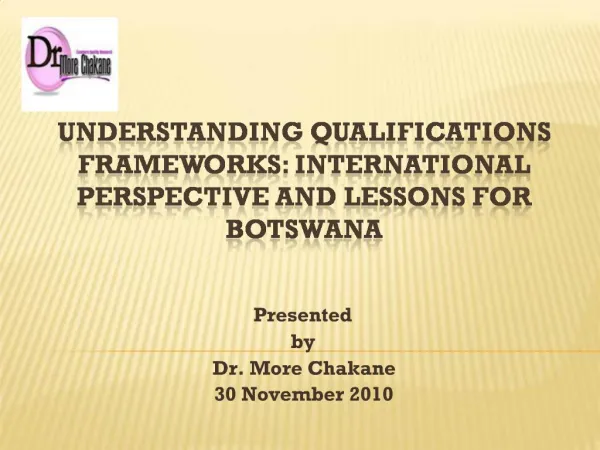
Solidarity? Cfr health care expenses 100,00 90,00 80,00 70,00 60,00 cumulative percentage of health care costs 50,00 40,00 30,00 20,00 10,00 0,00 0,00 10,00 20,00 30,00 40,00 50,00 60,00 70,00 80,00 90,00 100,00 sample Belgium population ranked according to medical consumption
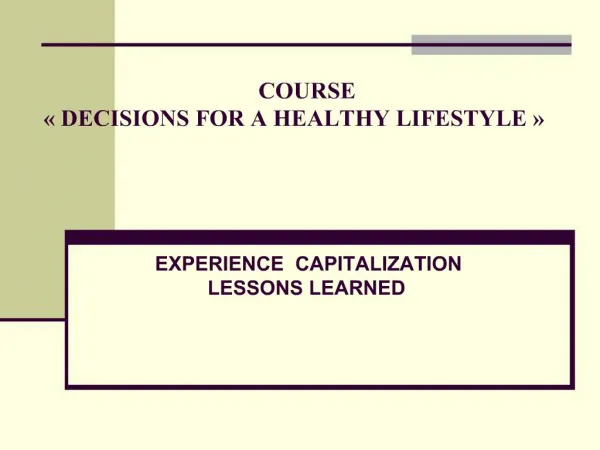
Three layer health care Prevention, cure and care not covered by public insurance Regulated competitionbetween insurers Package 2: cost-effective prevention and treatment, not in package 1 Package 1: primary prevention, screening, family and elderly care, chronic diseases No competitionbetween insurers W. Demeester, 1999
Content • Recommendations for improved health (care) policy (VGR) • Similarities and differences with Can/Den • Towards a blueprint for a Flemish health system • Objections against decentralization • Final thoughts
Objections (yes, but...) • What about Brussels? • Option 1: population chooses (cfr education • Option 2: Brussels as a separate entity (own health challenges; same size of several Canadian provinces) • What about the RIZIV/INAMI? • Transition to regional health agencies, responsible for steering (layer 1), regulating (layer 2) and facilitating (layer 3) • Feasibility and plan to be established with RIZIV/INAMI top • Cross-border care? • Cfr. European legislation with this regard • What about solidarity? See earlier argumentation • Plus: see Figures about affordability in Denmark • Why not recentralizing? See next slide
Why recentralization is less of an option • Are we then going to recentralize social services, labour, education, …? If not, the same problems remain; if yes, decreasing efficiency in those fields • Regional models have succeeded in improving efficiency; making the system more patient-oriented; and enhancing cost-consciousness (Bergman, 1998) • Centralization hinders integrated care, leads to information overload and being out of touch with providers (adversely affecting motivation, and makes it difficult to respond to complex local conditions (Mur-Veeman, 2008) • HOWEVER: limits to decentralization • Cfr HTA in Canada (CCADTH), • Cfr. NBOH’s role in Denmark • Cfr. Health information system in Canada (CIHI)
Content • Recommendations for improved health (care) policy (VGR) • Similarities and differences with Can/Den • Towards a blueprint for a Flemish health system • Objections against decentralization • Final thoughts
Final thoughts • Decentralization is not strange nor unrealistic • “Whatever the approach, strong leadership and trust are required for effective planning and sustainability”. (Stoto, 2008) (the devil lies in the detail) • Two attitudes: • Decentralization as goal • “decentralization makes everything better” • Decentralization as a means • “many recommendations for improving our health care can be made; with a decentralization, most of these recommendations can be better realized” (VGR, 2006) • Equity means solidarity based on objective criteria and does not mean supporting inefficiency (cfr unjustified overconsumption)
Lessons from the “Canadanish” experienceTHANK YOU Lieven Annemans Universiteit Gent, VUB