Download
1 / 20
330 likes | 910 Views
Nonalcoholic Fatty Liver Disease. s_khalilzadeh. A Novel Cardiometabolic Risk Factor for Type 2 Diabetes. NAFLD and T2DM. NAFLD is closely associated with features of the metabolic syndrome and is regarded as the hepatic manifestation

E N D
Nonalcoholic Fatty Liver Disease s_khalilzadeh
NAFLD and T2DM • NAFLD is closely associated with features of the metabolic • syndrome and is regarded as the hepatic manifestation • of the syndrome .The amount of intrahepatic • fat closely correlates with serum liver enzyme levels and • the number of metabolic syndrome features Patients • with T2DM have approximately 80% more intrahepatic • fat content than age-, sex-, and body weight-matched nondiabetic Controls, and their serum liver enzymes are less • representative of the severity of intrahepatic fat accumulation
NAFLD AND T2DM • patients with NAFLD and T2DM are • also more likely to develop the more advanced forms of • NAFLD, such as NASH, advanced fibrosis, cirrhosis, and • in some cases hepatocellular carcinoma
Poor glycemic control • Because NAFLD is strongly associated with IR, patients • With T2DM and NAFLD often have poor glycemiccontrol • compared to their counterparts without NAFLD • The presence of NAFLD in people with T2DM often • makes it difficult to obtain good glycemic control
stable glycemic controlwith in insulin treated T2DM patient it has • been demonstrated that the intrahepatic triglyceride content • was more closely correlated with the daily insulin dose • and the ability of insulin to suppress hepatic glucose production • and better explained the interindividual variation • in insulin requirements
In addition, when the relationship between NAFLD • and peripheral glucose metabolism was explored in • healthy individuals, the association between the intrahepatic • triglyceride content and systemic IR was stronger • than the association with intramyocellular lipid content, • visceral fat content, or sc fat content
NAFLD and risk of chronic diabetic complicationsand mortality among T2DM patients • The presence of NAFLD among patients with T2DM • appears to be an important risk factor for all-cause mortality. • A community-based study of T2DM individuals • reported that those with NAFLD had a 2.2-fold increased • risk of all-cause mortality compared with those • without NAFLD; the most common causes of death • were malignancy, CVD, and liver-related complications • Evidence is mounting that NAFLD is associated • with the presence of vascular disease, ie, the most common • cause of death in people with T2DM
Evidence Linking NAFLD With Risk ofDeveloping T2DM • modestly increased serum GGT and ALT levels were independent, • long-term predictors of incident T2DM in • both sexes
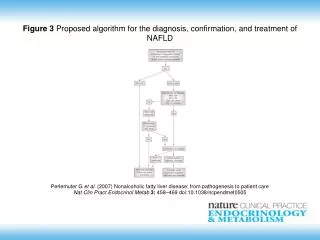
Treatment Options for NAFLD • Presently, there is no licensed treatment for humanNAFLD • Most interventions evaluated for the treatment • of NAFLD are those commonly used for the treatment of • T2DMand exert a rather indirect effect through improvement • in IR and glycemia
Statins • statins can be used in dyslipidemic individuals with increased • baseline liver enzymes and may even produce • Some histological benefit in NASH
Lifestyle modifications • gradual weight reduction, • achieved either by hypocaloric diet alone or in combination • with increased physical exercise, can be effective in • decreasing hepatic steatosis and necroinflammation (the • reduction of hepatic steatosis and necroinflammation is • proportional to the intensity of the lifestyle intervention • and generally requires a weight loss between 5 and 10%)
Insulin-sensitizing agents • Metformin, the first-line choice in oral therapy for • T2DM, has beneficial effects on serum aminotransferases • and IR but has no significant effect on liver histology and • is not recommended as a specific treatment for liver disease in patients with NAFLD/NASH
Insulin-sensitizing agents • Pioglitazone can • be used to treat steatohepatitis in patients with biopsyproven NASH; • there are no randomized clinical trials with • histological endpoints that investigated pioglitazone to • specifically t reat patients with NAFLD. A recent metaanalysis • reported that pioglitazone improved steatosis and • necroinflammation, but not fibrosis
Omega-3 polyunsaturated fatty acid (PUFA)supplementation • supplementation • High doses of omega-3 PUFAs are effective in treating • hypertriglyceridemia that is often a feature of NAFLD and • T2DM.
Glucagon-like peptide agonist (GLP-1 analog) • GLP-1 agonists have proved to be effective therapies to • improve glycemic control in people with T2DM; and interesting • additional effects of treatment are weight loss, • decreased appetite, and improved IR, which can prove • helpful in people with NAFLD
Vitamin E • It is known that increased oxidative stress occurs in • Both NAFLD and T2DM .Consequently, besides targeting • IR or lipid synthesis mechanisms per se, another therapeutic • option for NAFLD treatment may be to decrease • oxidative stress by administration of an antioxidant such • as vitamin E. Vitamin E therapy, as compared with placebo, • was associated with significant improvements in liver enzymes • and some histological features of NASH such as • steatosis and necroinflammation
Vitamin D • Preliminary experimental evidence • suggests that via effects in both adipose tissue and liver, • low serum vitaminD levels may predispose to intrahepatic • lipid accumulation and hepatic inflammation, contributing • to the development and progression of NAFLD • . However, whether vitamin D supplementation ameliorates • NAFLD is uncertain, and randomized clinical • trials are needed in man.