Download
1 / 86
870 likes | 1.19k Views
Septic and crystal arthritis. Jaya Ravindran Rheumatologist. Case 1. 82 year old Admitted 2.6.08 acute on chronic knee pain 3-4 days Recent excision of shin BCC with skin graft complicated by cellulitis Ex Not unwell afebrile MEWS O

E N D
Septic and crystal arthritis Jaya Ravindran Rheumatologist
Case 1 • 82 year old • Admitted 2.6.08 acute on chronic knee pain 3-4 days • Recent excision of shin BCC with skin graft complicated by cellulitis • Ex Not unwell afebrile MEWS O • Warm, slightly tender knee effusion, tolerating 90 flexion • ? Wound infection started on antibiotics • CRP 187
Radiological abnormality? Differential diagnosis? Further investigations? Management? Case 1
Case 1 • No organisms, scanty WBC • Pyrophosphate crystals • Low dose colchicine • CRP 42
Case 2 • DS 42 year old lady • PMH Crohns • Admitted 12.5.08 with onset of feeling hot and cold, D & V, headache 10 days ago • 3 days ago developed painful swelling left wrist, right knee and left ankle • SH Roadie, smoker – 10 roll-ups/day, lives with husband and son
Ex unwell,T38.5, p117/min, BP 116/64, RR20/min, satn 91% air, urine nad Tender swollen and red wrist, knee and ankle CXR ‘clear’ IMP septic Plan BC, analgesia, iv antibiotics, IVI Systolic dropped to 90 systolic Na 122 CRP 285, Blood gas P02 7, PCO2 7 PH 7.4 Transferred to WGH Case 2
Case 2 • Seen by rheumatologist joints aspirated • 13.5 blood cultures group A Strep, aspirate no growth, WBC • 15.5 vasculitic rash, low complement ?post Strep • 16.5 ECHO normal, CRP and joints settling • 17.5 Right pleuritic chest pain with rub
Case 2 • P02 8 treat for PE as well • 21.5 CTPA cavitating consolidation right lower lobe, hilar nodes, no PE • Still spiking ?empyema – nil aspirated,, no AFB in sputum, HIV negative, awaiting WBC scan
Case 3 • DB 45 year old man • PMH RA on sulphasalazine • 4 day history painful hot swollen red right big toe • Differential? • Investigations?
Case 4 • 82 year old man • PMH LVF,AF, TIA, BPH • DH Aspirin, bumetanide, ramipril, digoxin, statin • Referred with acute on chronic wrist pain needing MST • Pain was so severe that he asked next door’s dog to stop barking! • WBC 13, CRP 155, Cr 143, XR OA changes
Case 4 • Ex Well afebrile MEWS 0 • Tender warm swollen right wrist • Dry tap • Imp ? Crystal • Oral prednisolone • Good response but then confused, t 37.5, p116/min, 3+ blood & 1+ prot urine dip, increasing painful swelling in left wrist and toe • Diagnosis and plan?
Case 4 • WBC 20, Cr 261 • MSU, BC and joint aspirated • IVI and antibiotics, MST and ramipril stopped • Uric acid crystals, no growth in aspirate • Wrists injected once presumed UTI treated • Wrists better, CRP 3, Cr 124
What are other differentials for monoarticular pain?
Monoarthritis - differential • Monoarticular sero-ve spondyloarthritis eg psoriatic and reactive arthritis • Monoarticular RA
Monoarthritis - differential • Haemarthroses (warfarin, bleeding disorders) • Trauma – fracture, internal derangement, haemarthroses
Others to think about • Osteonecrosis/AVN (steroids/alcohol/SLE) • Prosthetic joint - loosening, # or infection
Others to think about • Periarticular pathology • Cellulitis
Septic arthritis • 15-30 per 100,000 population • Fatal in 11% of cases in UK • Delayed or inadequate treatment leads to irreversible joint damage
Who gets septic arthritis? • pre-existing joint disease • prosthetic joints • low SE status, IV drug abuse, alcoholism • diabetes, steroids, immunosuppression • Skin lesions e.g. ulcers, particularly in context RA often source of infection
Which organisms? • common organisms Staphylococci or Streptococcus • Elderly & immunocompromised gram -ve organisms
Which organisms? • Anaerobes more common with penetrating trauma • Pseudomonas - IV drug abusers • young adults - significant incidence gonococcal arthritis
Who gets septic arthritis? • poor prognostic features: older pre-existing joint disease & presence of synthetic material within joint
What are the signs and symptoms of septic arthritis?
Symptoms & signs of septic arthritis • Symptoms usually present for < 2/52 • Typically hot, swollen, red tender joint with reduced range of movement, difficulty weight bearing • Night and rest pain • Large joints more commonly affected than small • majority of joint sepsis in hip or knee • Systemic upset (MEWS)
Symptoms & signs of septic arthritis • In pre-existing inflammatory joint disease symptoms in affected joint(s), out of proportion to disease activity in other joints. • 10% of cases > one joint • presence of fever not reliable indicator
Women>men Menses, pregnancy 1-3% arthritis 1day- weeks after sexual encounter Migratory (70%), Tenosynovitis (70%), monoarthritis (32%), polyarthritis (10%) Fever, Dermatitis (pustules, vesicular, haemorrhagic bullae, mac.papular) Gonococcal arthritis
What investigations are useful in septic arthritis?
Investigations • Synovial fluid aspiration • gram stain/m,c,s • Absence of organism does not exclude septic arthritis • polarised light microscopy (crystals) • NB suspected prosthetic joint sepsis should ALWAYS be referred to orthopaedics
Investigations • Blood cultures • Significant proportion blood cultures + ve in absence of + ve synovial fluid cultures • FBC ESR & CRP • Absence of raised WBC, ESR or CRP does not exclude diagnosis of sepsis
Other investigations • CRP useful for monitoring response to treatment • Urate may be normal in acute gout • U+E & LFT – prognosis and influence antibiotic regime
Other tests? • Gonococcal - skin pustule - skin swab, urethral/cervical /rectal/throat swab, blood culture, joint aspirate • genitourinary or respiratory tract infection then culture sputum and CXR & MSU • If periarticular sepsis – appropriate swabs and cultures
Imaging • Plain X rays no benefit in diagnosis but form baseline for any future joint damage. May show chondrocalcinosis (pyrophosphate arthritis). • MRI sensitive for osteomyelitis and spinal involvement
Imaging • Ultrasound useful in guiding needle aspiration eg hip • White cell scanning helpful in diagnosing prosthetic sepsis
Spinal infection • Discitis – with destruction end plates
MEWS score? • Shock? • Multi-organ failure? • RESUSCITATION
Antibiotic treatment of septic arthritis • Local and national guidelines • Liaise with micro. guided by gram stain • Conventionally given iv for 2 weeks or until signs improve, then orally for around 4 weeks
Joint drainage & surgical options • medical aspiration, surgical aspiration via arthroscopy or open arthrotomy • Suspected hip sepsis – early orthopaedic referral – may need urgent open debridement
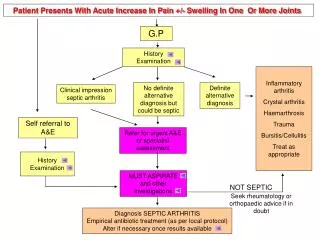
Recommendations specific to 1o care & emergency department • commonest hot joint to present in 1o care is 1st MTP gout • diagnosed on clinical grounds without needle aspiration or referral to hospital. (Make referral if inadequate recovery) • Some GPs aspirate & inject joints for inflammatory arthritis or osteoarthritis. If withdraw pus/unexpected cloudy fluid should send sample with patient to local emergency department
Recommendations specific to 1o care & emergency department • GPs & doctors in EAU should refer patients with suspected septic arthritis to specialist with expertise to aspirate joint. • May be orthopaedic surgeon or rheumatologist • Admit if sepsis is suspected or confirmed.
Summary • with a short history of a hot, swollen, tender joint (or joints) plus restriction of movement; septic arthritis until proven otherwise • If clinical suspicion high investigate & treat as septic arthritis even in absence of fever – always joint aspiration and blood cultures