Download
1 / 37
370 likes | 499 Views
Current State of Use of Evidence-Based Therapies for Acute Coronary Syndromes. Strategies to Improve Implementation of Guidelines-Based Care. Aspirin Clopidogrel Beta-Blocker ACE-Inhibitor Heparin ( UFH or LMWH ) GP IIbIIIa Inhibitor High-risk patients All receiving PCI. Aspirin

E N D
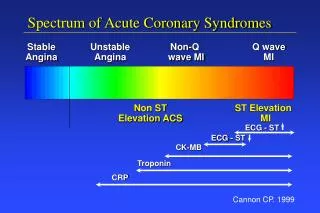
Current State of Use of Evidence-Based Therapies for Acute Coronary Syndromes Strategies to Improve Implementation of Guidelines-Based Care
Aspirin Clopidogrel Beta-Blocker ACE-Inhibitor Heparin (UFH or LMWH) GP IIbIIIa Inhibitor High-risk patients All receiving PCI Aspirin Clopidogrel Beta-Blocker ACE-Inhibitor Statin Smoking Cessation Cardiac Rehab AHA/ACC Guideline Recommendations Acute Therapy Discharge Therapy JACC 2000;36:970-1062 ACC/AHA 2002 Update
NRMI-4 NSTEMI Discharge Care: 3rd Quarter 2001 100% 84% 75% 80% 71% 56% 60% 40% 21% 20% 0% ASA Beta Blocker ACE Statins # Cardiac Inhibitor * Rehab * LVEF < 40% # Known hyperlipidemia
Gap between ‘Leading and Lagging’ US Hospitals Performance Quality Indicator Bottom 10% Top 10% ASA use < 24 h 54% 99% -blocker use < 24 h 33% 98% Heparin use <24 h 50% 92% GP IIb-IIIa < 24 h 0% 51% D/C ASA use 54% 99% D/C -blocker use 44% 96% D/C ACE-I use 21% 83% D/C lipid lowering 33% 99%
Evidence-Based Medicine:What’s the Problem? “There is an unsettling truth about the practice of medicine. …study after study shows that few physicians systematically apply to everyday treatment the scientific evidence about what works best.” Millenson, ML. Demanding Medical Excellence: Doctors and Accountability in the Information Age, 1997
Physician Barriers to Guidelines Adherence • Lack of awareness or agreement with guidelines • Lack of outcome expectancy • Uncertainty regarding impact of guidelines adherence on patient outcomes • Overcoming established practice patterns • External barriers to improved care • Time constraints, lack of resources, no reminders Cabana M, JAMA 1999
Benefits of Using Evidence-Based Therapies (Non-ST ACS Patients from GUSTO IIb) Additional Lives Current Use Saved per 1,000 Therapy (ideal pts) (ideal use) Aspirin 86% 9 Beta-Blockers 59% 11 ACE-Inhibitors 52% 23 Ca2+ Blockers * 27%* 13 Total 56 * Contraindicated use in low EF pts Ideal benefits from 0% use Alexander K, JACC, 1998
US News and World Reports’ “Top Ranked Hospitals” p < 0.01 Chen J, NEJM, 1999
Adherence to ACC/AHA Guidelines and Mortality:Results from NRMI-4 (n= 57,806 Acute MI patients, 1185 hospitals) 16 14 12 10 % In-hospital Mortality 8 6 4 2 0 30-50% 50-60% 60-70% >70% Rate of Hospital Composite Adherence (13 Indicators) Peterson E, ACC 2002
Local Quality Improvement Initiative Francis M. Fesmire, MD Erlanger Medical Center Chattanooga, TN
Erlanger QI Project - Objectives • Determine early utilization of GP IIb-IIIa inhibitors use in ED in high-risk NSTE ACS patients • Implement stepped QI program • Re-measure effectiveness of QI program
Erlanger QI Project - Methods • Prospective Observational Study • 2,074 patients presenting with chest pain • Patients not undergoing urgent cardiac cath underwent standard Chest Pain Evaluation Protocol at Erlanger
Erlanger QI Project - Interventions • Control (months 1-4): No intervention • Phase I (months 5-8): Posted eligibility criteria for GP IIb/IIIa inhibitors in ED • Phase II (months 9-12): Mandated QI form for completion by the evaluating ED physician with weekly review and feedback
Erlanger QI Project - Results (1) • % of patients who received GP IIb/IIIa inhibitors: • Control Phase: 6% • Phase I QI Intervention: 16% • Phase II QI Intervention: 45%
Erlanger QI Project - Results (2) • Reasons for not treatment in Phase II • 63% - ED Physician Never Realized Eligibility • 24% - Treatment was perceived to delay transfer to the cardiac cath lab • 10% - Admitting Physician did not want GP IIb/IIIa inhibitors to be administered • 3% - Contraindication
UCLA Cardiovascular Hospitalization Atherosclerosis Management Program (CHAMP) Gregg C. Fonarow, MD; Anna Gawlinski, DNSc Am J Cardiol 2000;85:10A-17A Am J Cardiol 2001;87:819-822
CHAMP - Program Overview (1) • CHAMP focused on the in-hospital initiation of: • Aspirin • Cholesterol-lowering therapy (statins) • Beta-blockers • ACE-Inhibitors • Medical interventions were done together with diet, exercise, and smoking cessation counseling before discharge in patients with acute MI Am J Cardiol 2000;85:10A-17A
CHAMP - Program Overview (2) • Implementation of CHAMP involved the use of: • Focused treatment guidelines • Standardized admission orders • Educational lectures by local thought leaders • Tracking and reporting of medication treatment rates • Treatment rates and clinical outcomes were compared in patients with acute MI discharged in the 2-year periods before and after CHAMP was implemented Am J Cardiol 2000;85:10A-17A
Medication Utilization Rates at Discharge Pre-CHAMP Post-CHAMP (1992-1993) (1994-1995) Discharge Therapy (n=256)(n=302) p-value Aspirin 78 92 <0.001 Beta-Blockers 12 61 <0.001 Nitrates 62 34 <0.01 Calcium Antagonists 68 12 <0.001 ACE-Inhibitors 4 56 <0.001 Statins 6 86 <0.0001 Am J Cardiol 2000;85:10A-17A
CHAMP - Sustained Impact Over 6 Years UCLA 77 59 41 28 NRMI Data from UCLA compared to 1437 other NRMI Hospitals
Regional Quality Improvement Initiative:The Guidelines Applied in Practice (“GAP”)Initiative in Southeast Michigan Kim A. Eagle, M.D.University of Michigan
Partnership ACC • GAP Committee • AMI Committee MPRO GDAHC • Greater Detroit Area Health Council • Employers, Insurers Providers • Michigan Peer Review Organization • QI Network • Measurement
GAP Toolkit for AMI Care • Standard Orders • Pocket Guidelines Cards • Clinical Pathways • Patient Information Forms • Patient Discharge Forms (Flight plan) • Hospital Performance Charts • Chart Stickers
GAP Rapid Cycle Change Hospital Selection Major Results Presentation March 2001 February 2000 Project Kick-off Presentation January – February 2001 March 2000 Data Analysis September – December 2000 April- June 2000 March – September 2000 Hospital Remeasurement Individual Hospital Kick-off Project Implementation
GAP Results: Early Indicators (Aggregate) Time in Minutes * 150 100% * 130 87% 81% 111 74% 70% 80% 65% 64% 100 60% 40 40% 38 50 20% 0 0% (40) (24) (32) (45) (343) (404) (213) (245) (131) (252) LYSIS PTCA BB LDL CHOL ASA PRE POST * p < 0.05 ** p < 0.01
GAP Results: Late Indicators (Aggregate) ** 93% 92% 100% 86% 89% 84% 80% 75% * 80% 68% 65% 53% 60% 40% 20% 0% (267) (406) (106) (146) (139) (173) (159) (226) (112) (209) ASA BB ACE SMOKING CHOL RX PRE POST * p < 0.05 ** p < 0.01
GAP Conclusions • Performance regarding early quality indicators is enhanced when AMI-specific standard ordersets are used • Adherence to late quality indicators is enhanced by use of an AMI-specific standard discharge tool • Further studies are underway to compare the performance levels achieved in GAP hospitals to non-GAP hospitals in the region
Challenges to Improved Patient Care Lack of use of best treatments Poor knowledge of best treatments Lack of systems to collect and understand clinical information Lack of knowledge of how to influence practice
The Cycle of Clinical Therapeutics Concept Clinical Trials Guidelines Outcomes Performance Indicators Performance
Process of Continuous Quality Improvement (CQI) Mobilization Identify Physician Champions Establish Local Consensus Feedback Intervention Review local treatment data Determine need for improvement Develop targeted interventions Planning Local Education Develop Hospital Plan Build Local QI Team Implementation Collect Baseline Data Care Pathways
Strategies to Improve Patient Care • Physician Continuing Medical Education • Local Opinion Leaders/Champions • Regular Feedback on Performance • Reminders, Care Pathways, Algorithms • Patient-Oriented Interventions • Total Quality Management - Multifaceted Interventions Grol R, JAMA 2001
Quality Improvement Interventions:Predictors of Success • Shared goals among health care providers regarding use of evidence-based therapies • Administrative support for CQI projects • Strong leadership by physician “champions” for improved patient care • High-quality data feedback mechanisms Bradley E, JAMA 2001 - Use of Beta-Blockers Post-MI
Practical Steps to Improve the Use of Evidence-Based Therapies for Non-ST ACS • Improve physicians’ knowledge of the ACC/AHA practice guidelines • Encourage cooperation between Emergency Medicine physicians and Cardiologists • Accurately track adherence to treatment recommendations from the guidelines • Secure institutional commitment to improved patient care with guidelines implementation
Steps for Improved ACS Care • Utilize simple data collection tools • Encourage multi-disciplinary collaboration • Study entire spectrum of ACS • Continuously update clinical practice guidelines • Mandate quality monitoring for all hospitals • Tie financial reimbursement to quality of care