Download
1 / 48
540 likes | 1.31k Views
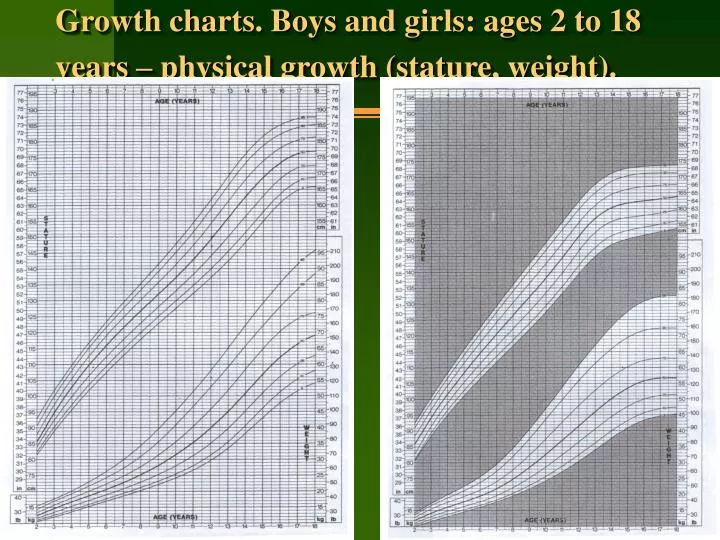
Growth charts. Boys and girls: ages 2 to 18 years – physical growth (stature, weight). If a variety of measurements such as weight, length or HC are assessed, then a normal bell-shaped distribution curve is found.

E N D
Growth charts. Boysand girls: ages 2 to 18 years – physical growth (stature, weight).
If a variety of measurements such as weight, length or HC are assessed, then a normal bell-shaped distribution curve is found. • The measurements are distributed symmetrically on each side of the mean, with a larger cluster around the mean. • Such a typical distribution curve can also be presented as a percentile chart.
Height Velocity • It is calculated from at least two accurate readings at a gap of 6 months (preferably one year). • A velocity of less than 4 cm per year between 5 years of age and adolescence is considered pathologic.
Percentiles • A specific point in a distribution curve which has a given percentage of cases above and below it. • The 50th percentile is seen as the midpoint of a normal distribution curve with 50 % of cases above and 50 % of cases below it. • The lower limit of normal is taken for practical purposes as the 3rd percentile and the upper limit as the 97th percentile. Only 3 % of normal cases fall below the 3rd percentile and 3 % above the 97th percentile.
A flat curve • It indicates a slowed or arrested growth which must alert the doctor to take action – both diagnostics and corrective.
The growth chart is primarily meant for the mother, to visualize and motivate concern for healthy growth in her child.
Body Ratios • They can be established by the mean of different indexes: • The index of fatness by Chulitska • The index by Erismann • Weight-for-height index • Height-for-age index • Stem stature index • Span
Weight-for-height index • Percentage weight-for-height = Actual weight 100 divided by Expected weight for actual height
Height-for-age index • Percentage height-for-age = Actual height 100 divided by Expected height for child’s age
Stem stature index • Refers to the sitting height (crown-rump length) as a percentage of the total height: I = SH/H 100 % • Its normal values are:
Stem stature index • This index is increased in hypothyroidism and dwarfism (achondroplasia).
Span • It is the distance between tips of middle fingers when the arms are outstretched. • It is equal to height at 10 years. • In earlier years, it is 1 to 2 cm less than the height. • After 12 years, it is 1 to 2 cm more then height. • It is increased in spondyloepiphyseal dysplasia (Morquio disease).
Standard deviation (SD) • Refers to the degree of dispersion of observations around the “mean”. • The prefix (+) to the SD value indicates a dispersion to higher side whereas the prefix (-) denotes the same to lower side. • 1 SD signifies that about 68 % observations lie within this range. • 2 SD includes about 95 % • 3 SD as high as 99.7 % of the cases.
Minor deviations of physical development (growth) • Failure to thrive • Short stature
Failure to Thrive • It is applied to infants and young children usually upto the age of 2 or 3 years, who show failure of expected growth (usually weight gain) and striking lack of wellbeing. • Simply put it describes a failure of expected normal growth and well-being. • Remember that it is a descriptive and not diagnostic term.
Failure to Thrive • It is also often used as synonym with the psychosomatic growth failure or maternal deprivation syndrome. • Etiology: • Poor nutritional intake and feeding problems. • Poverty, ignorance and conflict in the family. • Parental neglect. • Intestinal parasites infesting the child’s gut. • Increased loss through vomiting or malabsorption. • Poor utilization of food secondary to an underlying organic condition (e.g. Congenital heart desease) or chronic illness.
Short stature • It is the equal delay of height and weight gain in children in comparison to the average data. The height-weight velocity curves of such children are within the 2nd and the 3rd percentiles. • Etiology of small stature is heredity, lack of protein and vitamins intake during prenatal period and the 1st year of life.
Short stature • Types: • Primary short stature is usually due to an intrinsic defect in the sceletal system as a result of some genetic or prenatal damage (IUGR). Here, potential for normal bone growth is impaired though skeletal age is unaffected. • Secondary short stature is characterized by impairment of bone age and height to the same extent.
Midparental height • The so-called midparental height, a genetic component, gives the subject’s target height. • It is determined as sum of father and mother’s heights plus 13 in case of boys and minus 13 in case of girls.
Major deviations of physical development (growth) • Hypotrophy • Paratrophy • Obesity • Nanism (dwarfism) • Gigantism
Protein-energy malnutrition(hypotrophia) It is a pathological state resulting from a severe deprivation, or impaired absorption, of protein or/and caloric food, which lead to weight reduction, wasting of subcutaneous fat and muscle, and stunting.
Classification of protein-energy malnutrition (hypotrophia) • Primary, when there is deficiency of food availability: • failure of lactation; • ignorance of weaning; • poverty and starvation; • cultural patterns and food fads; • lack of primary care; • lack of family planning.
Secondary, when food is available but body can not assimilate it for one or another reason: • infections; • congenital diseases; • malabsorption (lactose intolerance, celiac disease, cystic fibrosis); • inborn errors of metabolism (fenylcetonuria, galactosemia, diabetes mellitus, diabetes insipidus, storage diseases); • psychological deprivation.
Prenatal (congenital): it leads to birth of low-weight-birth babies. • Aquired: as a rule, develops after 3rd month of child’s life.
Anthropometric classification of protein-energy malnutrition (hypotrophia )
Clinical classification of protein-energy malnutrition 2 main syndromes: • Marasmus • Kwashiorkor
Marasmus • Predominates in infancy (below 2 years of age) ; • Most commonly results from a severe deprivation of food intake (lack of both proteins and energy; • Clinical features: • marked loss of subcutaneous fat and muscles; • growth retardation; • skin is loose and hangs in folds; • abdomen is protuberant; • face is like “little old man” or monkey face; • hypothermia; • child is usually alert, irritable and has a good appetite; • edema is never present.
Wasting means marked loss of muscle and subcutaneous tissue. • Stunting is a term introduced by Waterlow to describe the profound effect of nutritional deprivation on linear growth.
Kwashiorkor • It usually occurs between 1-5 years of age. • It results from inadequate protein intake. • Clinical features: • generalized edema; • wasting masked by edema: thin lean muscles, some fat is present; • skin lesions: Flaky-Paint dermatitis; • hair changes: hair thin, sparse, depigmented (grayigh or reddish), dull; • apathy; • anorexia; • hepatomegaly resulting from fatty infiltration of the liver; • anaemia: due to low iron stores and low protein supply.
Kwashiorkor in a 2-yr-old boy. Note the generalized edema, the typical skin lesions, and the state of prostration. Close-up of the same child showing the hair changes and psychic alterations (apathy and misery); the edema of the face and the skin lesions can be seen more clearly.
Paratrophy • It is enlargement of body weight more than for 10 % of ideal weight. The main course of it is overfeeding of a baby. • According to clinical signs paratrophy is divided into 2 types: lipomatic and lipomatic-pastose. • In case of lipomatic type the child looks healthy (skin and mucous membranes are of nature colour, turgur is normal, etc); laboratory tests are normal. The child gets ill rarely and for a shot period. • In case of lipomatic-pastose paratrophy skin is pale, flabby and edematic, turgur is decreased, signs of anemia are present. The child is dull mood and not active. On the first year of life such children often have allergic reactions, rickets, weakened immune system (often acute respiratory infections).
Obesity • The presence of excessive weight in child older than 1 year is called obesity.
Nanism (dwarfism) • It is a disorder of physical development, which deals with the delay of height below the 3rd percentile for age according to international standard or 3 standard deviations of mean for age. • The dwarf height in adult persons of white race is considered the height below 130 cm for male and below 120 cm for female.
Classification: • dwarfism with proportional constitution; • dwarfism with disproportional constitution.
Dwarfism Etiology of nanism is congenital disorders of endocrine system (hypofunctions of hypophysis or thyroid) or metabolism. • If weight is less proportionally reduced than height nutritional deprivation must be seriously considered. • If weight is nearly normal but height is significantly less, hypothyroidism must be seriously considered. • Growth hormone deficiency and hypercorticism also figure in the differential diagnosis. • Present signs of delayed puberty arouse suspition of sex chromosomal anomalies (e.g. Turner syndrome).
Common Pituitary Disorders (cont’d): Hypopituitarism (pituitary dwarfism) • Clinical Manifestations: 1. Weight loss. 2. Atrophy of all endocrine glands and organs. 3. Hair loss. 4. Impotence. 5. Amenorrhea. 6. Hypoglycemia. • Treatment: - Replacement of missing hormone (as GH)
Young female dwarf standing next to a boy of normal stature. (Photograph by Dr. Richard Pauli. U. of Wisconsin, Madison, Clinical Genetics Center.)
Gigantism • It’s a clinical syndrome, which develops as a result of hyperproduction of somatotropine hormone of hypophysis that leads to remarkable growth in height. • The first manifestation of gigantism takes place during prepubertal or pubertal periods. Other complaints are weakness, often headaches, extremity or cardiac pains. • Physical development of such children is disproportional: the height velocity goes up over the 3rd percentile, weight lies within the 2nd and 3rd percentiles and other measurements within “normal curves”.
That’s all for today, folks !! Any Qs?