Download
1 / 8
290 likes | 1.36k Views
Umbilical Cord Prolapse. Risk Factors Malpresentation, prematurity, polyhydramnios, high presenting part, long cord Epidemiology. Rapid Response to Prolapse. Recognize non-reassuring tracing Visually inspect/palpate cord to diagnose Assess fetal status (FHTs, ultrasound)

E N D
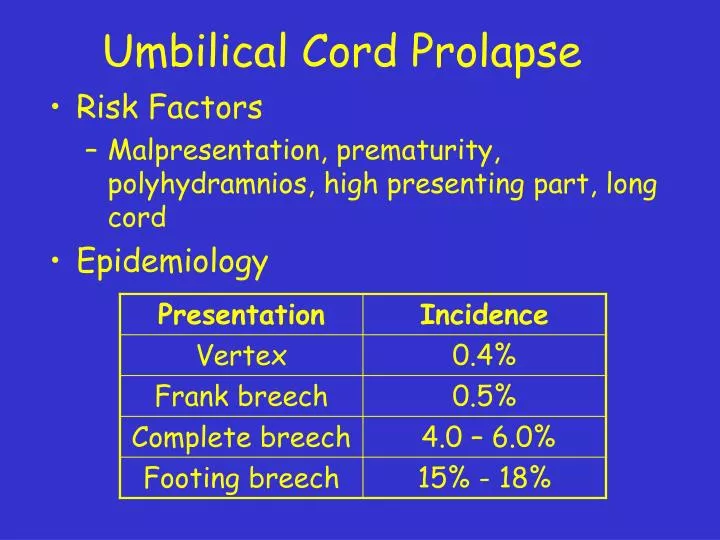
Umbilical Cord Prolapse • Risk Factors • Malpresentation, prematurity, polyhydramnios, high presenting part, long cord • Epidemiology
Rapid Response to Prolapse • Recognize non-reassuring tracing • Visually inspect/palpate cord to diagnose • Assess fetal status (FHTs, ultrasound) • Assess labour progress (dilation, station) • Do not attempt to replace cord • Hold presenting part off cord • Foley catheter • Position change (Trendelenburg, Knee-chest) • Tocolysis
Prevention of Prolapse • Identify risk factors • Malpresentation, high presentation • Patient education re: membrane rupture at home • No AROM when station high • May “needle” membranes under double set-up
Multiple Gestation • Occurs in 1.5% of U.S. births • 2-5 X higher perinatal morality • Maternal complications common • HTN, anaemia, hyperemesis, abruption, praevia, PPH, operative delivery • Dizygosity (fraternal) = 2/3 • Increases with age, parity, familial factors • Monozygosity (identical) = 1/3
Diagnosis of Multiple Gestation • Ovulation induction • Family history • Hyperemesis • Uterine size > dates • Early PIH • Elevated MSAFP • Auscultation of > 1 fetal heart beat • Polyhydramnios
Associated Complications • Prematurity • Congenital anomalies • Pregnancy-induced hypertension • Placenta praevia • Fetal death: 0.5% - 6.8%
Delivering Twin B • Attempt internal podalic version • Breech delivery is reasonable choice when: • External version unsuccessful or not attempted • Strong labour and Baby B deep in pelvis • Cord prolapse or nonreassuring FHR tracing
Summary • Six types of malpresentations • Diagnosis by physical exam and imaging • Be alert to etiologic association • Be alert to potential complications • Vaginal delivery may be considered for OP, breech, face and compound presentation