Download
1 / 13
260 likes | 1.02k Views
Guillain-Barre’. Guillain-Barre’ Syndrome. Post-infectious polyneuropathy; ascending polyneuropathic paralysis An acute, rapidly progressing and potentially fatal form of polyneuritis. Guillain-Barre’ Syndrome. Affects the peripheral nervous system. Guillain-Barre’.

E N D
Guillain-Barre’ Neurology Chapter of IAP
Guillain-Barre’ Syndrome • Post-infectious polyneuropathy; ascending polyneuropathic paralysis • An acute, rapidly progressing and potentially fatal form of polyneuritis Neurology Chapter of IAP
Guillain-Barre’ Syndrome • Affects the peripheral nervous system Neurology Chapter of IAP
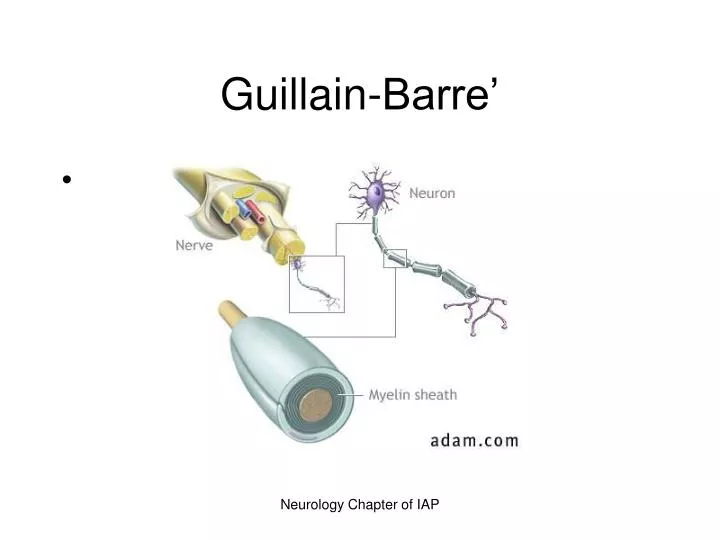
Guillain-Barre’ • T-cell sensitization occurs which causes loss of myelin which disrupts nerve impulses • Loss of myelin, edema and inflammation of the affected nerves, causes a loss of neurotransmission to the periphery. • 85% of patients recover with supportive care. Neurology Chapter of IAP
Pathophysiology • Etiology unknown • May be cell-mediated immunological reaction directed at the peripheral nerves • Frequently preceded by viral infection, trauma, surgery or other immune system stimulation. Neurology Chapter of IAP
Myelin Sheath Neurology Chapter of IAP
Clinical Manifestations • Usually develop 1 to 3 weeks after URI or GI infection • Weakness of lower extremities (symmetrically) • Parathesia (numbness and tingling), followed by paralysis • Hypotonia and areflexia (absence of reflexes) • Pain in the form of muscles cramps or hyperesthesias (worse at night). Neurology Chapter of IAP
Clinical manifestations • Autonomic nervous system dysfunction results from alterations in sympathetic and parasympathetic nervous systems. • Results in respiratory muscle paralysis, hypotension, hypertension, bradycardia, heart block, asystole. • Involvement of lower brainstem leads to facial and eye weakness Neurology Chapter of IAP
Complications • Most serious is respiratory failure. • How do we manage? Neurology Chapter of IAP
Diagnostic studies • Based on history and physical • EMG and nerve conduction studies will be abnormal Neurology Chapter of IAP
Therapeutic management • Ventilator support! • Plasmapheresis used within the first 2 weeks of onset. If treated within the first 2 weeks, LOS of morbidity is reduced. After three weeks, plasmapharesis no benefit. • IV immunoglobin • Nutritional support (TF, TPN, Diet) Neurology Chapter of IAP
Nursing management • See handout! • Read Nursing Implementation: Lewis, 1607-1608. Neurology Chapter of IAP